

A cross-lagged study of somatic symptoms and mental states in patients with chronic heart failure
-
摘要:
目的 采用交叉滞后回归分析模型探究慢性心力衰竭(chronic heart failure, CHF)患者躯体症状与心理状态之间的相互作用。 方法 选取2017年11月—2018年12月在山西省2家三甲医院心内科住院的262名慢性心衰患者,进行6个月的纵向追踪。采用心力衰竭患者报告结局调查问卷(patient-reported outcome measure for chronic heart failure, CHF-PROM)先后2次进行测量(T1和T2),采用交叉滞后回归模型分析躯体症状和心理状态之间的关系。 结果 慢性心力衰竭患者躯体症状和心理状态均具有一定稳定性。2次测量的躯体症状和心理状态均成正相关(r=0.331, P < 0.001; r=0.445, P < 0.001)。交叉滞后回归分析显示,控制T1躯体症状后,T1心理状态可以预测T2躯体症状(β=0.163, P=0.010);进一步分析心理状态各维度显示,控制T1躯体症状后,T1焦虑可以预测T2躯体症状(β=0.183, P=0.004)。 结论 心理状态是躯体症状的前因变量,心理状态可以正向预测躯体症状。进一步分析显示,焦虑是躯体症状的前因变量,焦虑对躯体症状具有正向预测作用。 Abstract:Objective The cross-lagged regression model was used to investigate the interaction between somatic symptoms and mental states in patients with chronic heart failure (CHF). Methods A six-month longitudinal follow-up was conducted amongst 262 patients with chronic heart failure who were admitted to the Department of Cardiology of two of the top three hospitals in Shanxi Province from November 2017 to December 2018. The patient-reported outcomes instrument for CHF (patient-reported outcome measure for chronic heart failure, CHF-PROM) was used for two measurements (T1 and T2), Cross-lagged regression model was used to analyze the relationship between somatic symptoms and mental states. Results The physical symptoms and mental states of patients with chronic heart failure were stable. There was a positive correlation between physical symptoms and mental states (r=0.331, P < 0.001; r=0.445, P < 0.001). Cross-lagged regression analysis showed that after controlling for T1 somatic symptoms, T1 mental states could predict T2 somatic symptoms (β=0.163, P=0.010); Further analysis of the psychological state of each dimension showed that T1 anxiety predicted somatic symptoms of T2 (β=0.183, P=0.004) after controlling for T1 somatic symptoms. Conclusions Mental states are the antecedents of somatic symptoms, which can positively predict somatic symptoms. Further analysis showed that anxiety is the antecedent variable of somatic symptoms and anxiety has a significant positive predictive effect on somatic symptoms. -

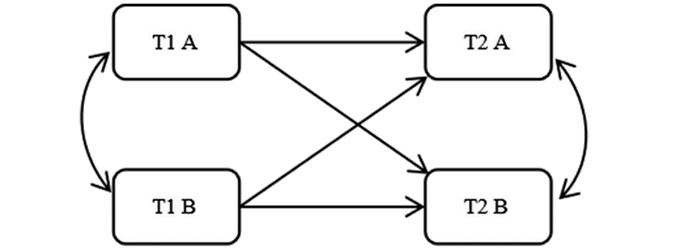
图 1 交叉滞后模型
注:T1表示前测,T2表示后测;双箭头表示相关系数,单箭头表示路径系数;单箭头实线表示路径系数有统计学意义。
Figure 1. Cross-lagged regression

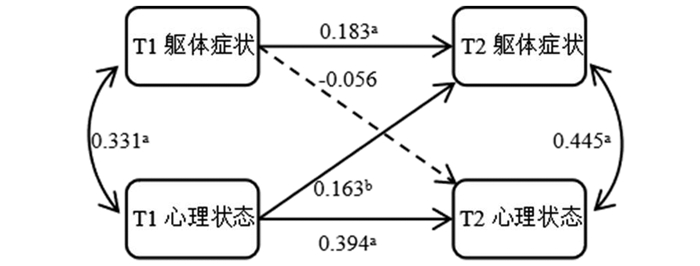
图 2 躯体症状与心理状态的交叉滞后回归分析模型
注:T1表示前测,T2表示后测;a表示P < 0.01,b表示P < 0.05;双箭头表示相关系数,单箭头表示路径系数;单箭头实线表示路径系数有统计学意义,单箭头虚线表示无统计学意义。
Figure 2. Cross-lagged regression analysis of somatic symptoms and mental states

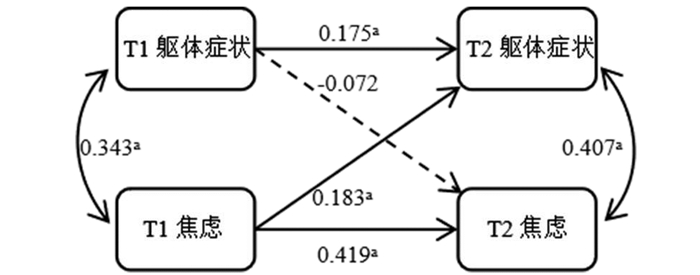
图 3 躯体症状与焦虑的交叉滞后回归分析模型
注:T1表示前测,T2表示后测;a表示P < 0.01,b表示P < 0.05;双箭头表示相关系数,单箭头表示路径系数;单箭头实线表示路径系数有统计学意义,单箭头虚线表示无统计学意义。
Figure 3. Cross-lagged regression analysis of somatic symptoms and anxiety
表 1 CHF患者的一般情况[n(%)]
Table 1. General situation of patients with CHF [n(%)]
变量 人数 百分比(%) 年龄(岁) < 55 49 18.7 55~ 43 16.4 65~ 69 26.4 ≥75 101 38.5 性别 男性 148 56.5 女性 114 43.5 婚姻状况 未婚 4 1.5 已婚 211 80.6 离异 4 1.5 丧偶 43 16.4 文化程度 文盲 22 8.4 小学 64 24.4 初中 96 36.6 高中(含中专) 38 14.5 大专 28 10.7 本科及以上 14 5.3 家庭收入 低 118 45.0 中 140 53.5 高 4 1.5 家族史 无 174 66.4 有 88 33.6 既往史 无 107 40.8 有 155 59.2 NYHA Ⅰ级 10 3.8 Ⅱ级 71 27.1 Ⅲ级 121 46.2 Ⅳ级 60 22.9  下载: 导出CSV
下载: 导出CSV
表 2 CHF患者躯体症状和心理状态及各维度得分情况(x±s)
Table 2. Scores of somatic symptoms, mental state and various dimensions in patients with CHF (x±s)
项目 T1(分) T2(分) 男 女 总体 男 女 总体 躯体症状 30.54±5.50 29.32±5.90 30.01±5.72 37.59±2.38 36.71±3.20 37.21±2.80 心理状态 91.55±11.82 84.71±13.21 88.58±12.88 101.73±3.96 99.41±6.62 100.72±5.40 焦虑 31.70±6.06 27.83±6.56 30.02±6.56 37.57±2.88 36.05±4.07 36.91±3.53 抑郁 26.80±4.24 24.87± 4.73 25.96±4.56 29.30±1.11 28.80±1.72 29.08±1.43 恐惧 13.89±1.70 13.19±2.44 13.59±2.08 14.86±0.45 14.71±0.94 14.80±0.71 偏执 19.16±1.88 19.16±1.88 19.01±2.09 19.99±0.07 19.85±0.90 19.93±0.60
下载: 导出CSV
表 3 躯体症状与心理状态的相关
Table 3. Correlation between somatic symptoms and mental state
项目 T1SOM T2SOM T1PSY T2PSY T1SOM 1.000 T2SOM 0.246a 1.000 T1PSY 0.331a 0.247a 1.000 T2PSY 0.086 0.445a 0.405a 1.000 注:a表示P < 0.01。
下载: 导出CSV
表 4 躯体症状与心理领域各维度的相关
Table 4. Correlation between somatic symptoms and dimensions of psychological field
项目 T1SOM T2SOM T1ANX T2ANX T1DEP T2DEP T1FEA T2FEA T1PAR T2PAR T1SOM 1.000 T2SOM 0.246a 1.000 T1ANX 0.343a 0.268a 1.000 T2ANX 0.083 0.407a 0.423a 1.000 T1DEP 0.211a 0.184a 0.670a 0.271a 1.000 T2DEP 0.086 0.380a 0.364a 0.739a 0.355a 1.000 T1FEA 0.274a 0.178a 0.543a 0.240a 0.667a 0.311a 1.000 T2FEA 0.013 0.337a 0.221a 0.442a 0.222a 0.605a 0.185a 1.000 T1PAR 0.228a 0.101 0.436a 0.125b 0.487a 0.142b 0.528a 0.098 1.000 T2PAR 0.068 0.306a 0.201a 0.304a 0.283a 0.543a 0.252a 0.812a 0.175a 1.000 注:a表示P < 0.01;b表示P < 0.05。
下载: 导出CSV
-
[1] Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC[J]. Eur Heart J, 2016, 37(27): 2129-2200. DOI: 10.1093/eurheartj/ehw128. [2] Heo S, Lennie TA, Okoli C, et al. Quality of life in patients with heart failure: ask the patients[J]. Heart lung, 2009, 38(2): 100-108. DOI: 10.1016/j.hrtlng.2008.04.002. [3] Zhang Y, Lv XZ, Jiang W, et al. Effectiveness of a telephone-delivered psycho-behavioural intervention on depression in elderly with chronic heart failure: rationale and design of a randomized controlled trial[J]. BMC Psychiatry, 2019, 19(1): 1-9. DOI: 10.1186/s12888-019-2135-2. [4] Sokoreli I, de Vries JJG, Pauws SC, et al. Depression and anxiety as predictors of mortality among heart failure patients: systematic review and meta-analysis[J]. Heart Fail Rev, 2016, 21(1): 49-63. DOI: 10.1007/s10741-015-9517-4. [5] Lichtman JH, Froelicher ES, Blumenthal JA, et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: systematic review and recommendations a scientific statement from the American Heart Association[J]. Circulation, 2014, 129(12): 1350-1369. DOI: 10.1161/CIR.0000000000000019. [6] Vongmany J, Hickman LD, Lewis J, et al. Anxiety in chronic heart failure and the risk of increased hospitalisations and mortality: a systematic review[J]. Eur J Cardiovasc Nurs, 2016, 15: 478-485. DOI: 10.1177/1474515116635923. [7] 薛江平. 慢性心衰PRO量表的研制与评价[D]. 太原: 山西医科大学, 2012.Xue JP. Development and evaluation of patient-reported outcomes instrument for chronic heart failure[D]. Taiyuan: Shanxi Medical University, 2012. [8] 吕静, 薛江平, 罗艳虹, 等. 慢性心衰PRO量表条目的初步筛选[J]. 中国卫生统计, 2014, 31(3): 379-382.Lv J, Xue JP, Luo YH, et al. Item screening about PRO scale of chronic heart failure[J]. Chin J Health Statistics, 2014, 31(3): 379-382. [9] Bollen KA, Curran PJ. Autoregressive latent trajectory (ALT) models a synthesis of two traditions. [J]. Sociol Methods Res, 2004, 32(3): 336-383. DOI: 10.1177/0049124103260222. [10] Bentler PM. Comparative fit indexes in structural models[J]. Psychol Bull, 1990, 107(2): 238-246. DOI: 10.1037/0033-2909.107.2.238. [11] Baik D, Reading M, Jia HM, et al. Measuring health status and symptom burden using a web-based mHealth application in patients with heart failure[J]. Eur J Cardiovasc Nurs, 2019, 18: 325-331. DOI: 10.1177/1474515119825704. [12] 李连江. 慢性心力衰竭诊断与治疗进展[J]. 中西医结合心血管病电子杂志, 2017, 5(22): 20. DOI: 10.16282/j.cnki.cn11-9336/r.2017.22.011.Li LJ. Progress in diagnosis and treatment of chronic heart failure[J]. Cardiovascular Disease Journal of integrated traditional Chinese and Western Medicine, 2017, 5(22): 20. DOI: 10.16282/j.cnki.cn11-9336/r.2017.22.011. [13] 王芳. 慢性心力衰竭患者症状负担对生活质量的影响及模型构建[D]. 蚌埠: 蚌埠医学院, 2016.Wang F. Effects of symptom burden on quality of life in patients with chronic heart failure and its construction of model[D]. Bengbu: Bengbu Medical College, 2016. [14] 黄红, 葛晓燕, 刘唯薇. 慢性心力衰竭患者焦虑抑郁影响因素分析[J]. 交通医学, 2020, 34(1): 78-79, 82. DOI: 10.19767/j.cnki.32-1412.2020.01.030.Huang H, Ge XY, Liu WW. Analysis of influencing factors of anxiety and depression in patients with chronic heart failure[J]. Med J Communications, 2020, 34(1): 78-79, 82. DOI: 10.19767/j.cnki.32-1412.2020.01.030. [15] 李中清, 潘发明. 充血性心力衰竭住院患者抑郁状态分析及心理干预效果评价[J]. 中华疾病控制杂志, 2012, 16(6): 502-505. http://zhjbkz.ahmu.edu.cn/article/id/JBKZ201206015Li ZQ, Pan FM. Analysis of depression state and the evaluation of mental intervention effect among patients with congestive heart failure[J]. Chin J Dis Control Prev, 2012, 16(6): 502-505. http://zhjbkz.ahmu.edu.cn/article/id/JBKZ201206015 [16] 赵英. 综合性护理干预在改善慢性心力衰竭患者焦虑状态中的应用效果观察[J]. 中国医药指南, 2015, 13(34): 238-239. DOI: 10.15912/j.cnki.gocm.2015.34.197.Zhao Y. Observation of application effect of comprehensive nursing intervention in improving anxiety state of patients with chronic heart failure[J]. Guide of China Medicine, 2015, 13(34): 238-239. DOI: 10.15912/j.cnki.gocm.2015.34.197. [17] 陈建华. 慢性心力衰竭患者焦虑状态的护理干预效果分析[J]. 中国社区医师, 2016, 32(14): 139-140. DOI: 10.3969/j.issn.1007-614x.2016.14.88.Chen JH. The effect of nursing intervention on anxiety state in patients with chronic heart failure[J]. Chinese Community Doctors, 2016, 32(14): 139-140. DOI: 10.3969/j.issn.1007-614x.2016.14.88. [18] 李丹. 慢性心力衰竭患者焦虑状态的护理干预效果分析[J]. 中国实用医药, 2018, 13(2): 149-150. DOI: 10.14163/j.cnki.11-5547/r.2018.02.089.Li D. The effect of nursing intervention on anxiety state in patients with chronic heart failure[J]. China Prac Med, 2018, 13(2): 149-150. DOI: 10.14163/j.cnki.11-5547/r.2018.02.089. [19] Schöner P, Horstkotte D, Piper C. Are psychological symptoms in patients with heart failure influenced by improvement of cardiological treatment?[J]. Psychother Psychosom Med Psychol, 2013, 63(7): 257-263. DOI: 10.1055/s-0032-1316385. [20] 李芳华, 刘国杰, 祁小红, 等. 老年慢性心力衰竭患者自我感受负担状况及其影响因素研究[J]. 护理学杂志, 2015, 30(19): 14-16, 34. DOI: 10.3870/j.issn.1001-4152.2015.19.014.Li FH, Liu GJ, Qi XH, et al. The self-perceived burden among elderly patients with chronic heart failure and its influencing factors[J]. J Nurs Sci, 2015, 30(19): 14-16, 34. DOI: 10.3870/j.issn.1001-4152.2015.19.014. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 362
- HTML全文浏览量: 301
- PDF下载量: 48
- 被引次数: 0