

Analysis on potential factors of small for gestational age of Zhuang ethnicity in Wuming District of Nanning
-
摘要:
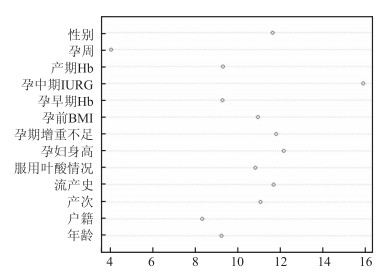
目的 了解壮族人群小于胎龄儿(small for gestational age,SGA)的流行情况,并探讨SGA的影响因素。 方法 选择2016年1月~2018年1月在南宁市武鸣区人民医院及武鸣区妇幼保健院产检并分娩的孕妇共3 839例,收集所有研究对象基本信息和相关研究因素的资料,采用随机森林算法、χ2检验和多因素Logistic回归对资料进行分析。 结果 武鸣区壮族人群SGA发生率为9.6%(368/3 839),其中男婴的发生率为6.9%(142/2 049),女婴的发生率为12.6%(226/1 790)。随机森林显示孕中期胎儿宫内生长受限(intrauterine growth retardation,IUGR)的重要性评分最高,孕周最低,并筛选了7个最重要的变量纳入多因素Logistic回归。多因素分析显示,初产妇、孕妇身高<1.55 m、孕期增重不足及孕中期IUGR是SGA的危险因素;孕前BMI ≥ 18.5 kg/m2及男婴则为SGA的保护因素。 结论 南宁市壮族人群SGA的发生率较高,且受多因素影响,应及时评估胎儿生长发育情况,采取综合措施以减少SGA的发生。 Abstract:Objective To understand the prevalence of small for gestational age (SGA) in Zhuang population, and to analyze the potential factors of SGA. Methods A total of 3 839 live births in the Wuming District People's Hospital and Wuming Maternal and Child Health Hospital from January 2016 to January 2018 were recruited. Random Forest, χ2 test and Logistic regression model were used for statistical analyses. Results The incidence of SGA was 9.6% (368/3 839), and it was 6.9% (142/2 049) and 12.6% (226/1 790) for male and female infants respectively. Random Forest method showed that second-trimester intrauterine growth restriction's importance score was the highest, but gestational week's was the lowest. Also, seven important variables were selected by this method. Unconditional logistic regression analysis showed that parity <2, the height of mothers <1.55 m, insufficient gestational weight gain, second-trimester intrauterine growth restriction were risk factors for SGA, but pre-pregnancy BMI ≥ 18.5 kg/m2 and male infants were protective factors. Conclusions The incidence of SGA is slightly higher, among the Zhuang population in Guangxi. SGA is affected by many factors. Therefore, it is necessary to evaluate the status of intrauterine growth and adopt comprehensive measures to control and reduce the incidence of SGA. -
Key words:
- Zhuang nationality /
- Infant /
- Small for gestational age /
- Risk factors
-
表 1 1武鸣区壮族孕妇基本特征[n(%)]
Table 1. Characteristics of pregnant women of Zhuang ethnicity in Wuming district [n(%)]
基本特征 SGA 非SGA χ2值 P值 年龄(岁) 0.035 0.851 <35 296(9.5) 2 806(90.5) ≥35 72(9.8) 665(90.2) 户籍 0.278 0.598 农村 335(9.7) 3 130(90.3) 城镇 33(8.8) 341(91.2) 产次 17.519 <0.001 初产 145(12.6) 1 003(87.4) 经产 223(8.3) 2 468(91.7) 流产史 5.579 0.018 有 170(8.5) 1 828(91.5) 无 198(10.8) 1 643(89.2) 是否服用叶酸 1.791 0.181 是 226(10.1) 2 006(89.9) 否 142(8.8) 1 465(91.2) 孕妇身高(m) 17.206 <0.001 ≥1.55 223(8.3) 2 465(91.7) <1.55 145(12.6) 1 006(87.4) 孕期增重不足 12.619 <0.001 否 253(8.6) 2 674(91.4) 是 115(12.6) 797(87.4) 孕前BMI(kg/m2) 17.244 <0.001 <18.5 70(14.9) 401(85.1) ≥18.5 298(8.8) 3 070(91.2) 孕早期Hb(g/L) 3.626 0.057 ≥110 281(9.1) 2 795(90.9) <110 87(11.4) 676(88.6) 是否孕中期IUGR 61.371 <0.001 否 275(8.2) 3 086(91.8) 是 93(19.5) 385(80.5) 产期Hb(g/L) 0.171 0.679 ≥110 290(9.5) 2 767(90.5) <110 78(10.0) 704(90) 孕周(周) 0.178 0.673 ≥37 360(9.6) 3 383(90.4) <37 8(8.3) 88(91.7) 新生儿性别 35.758 <0.001 男 142(6.9) 1 907(93.1) 女 226(12.6) 1 564(87.4)  下载: 导出CSV
下载: 导出CSV
表 2 壮族人群SGA多因素Logistic回归分析
Table 2. Multivariate logistic regression analysis of risk factors for SGA of Zhuang population
变量 β Wald值 P值 OR(95% CI)值 产次 经产 1.00 初产 0.484 16.889 <0.001 1.62(1.29~2.04) 孕妇身高(m) ≥1.55 1.00 <1.55 0.452 15.174 <0.001 1.57(1.25~1.97) 孕期增重不足 否 1.00 是 0.497 18.967 <0.001 1.64(1.31~2.06) 孕前BMI(kg/m2) <18.51.00 ≥18.5 -0.480 10.423 0.001 0.62(0.46~0.83) 是否孕中期IUGR 否 1.00 是 0.913 45.949 <0.001 2.49(1.91~3.24) 新生儿性别 女 1.00 男 -0.606 28.048 <0.001 0.55(0.44~0.68)
下载: 导出CSV
-
[1] Garcia-Basteiro AL, Quinto L, Macete E, et al. Infant mortality and morbidity associated with preterm and small-for-gestational-age births in Southern Mozambique: a retrospective cohort study[J]. PLOS ONE, 2017, 12(2): 0172533. DOI:10.1371/journal.pone.0172533.eCollection 2017. [2] 毛宝宏, 李静, 王燕侠, 等. 孕前及孕期叶酸摄入与小于胎龄儿的关联性分析[J]. 中国优生与遗传杂志, 2017, 25(9): 62-64. DOI: 10.13404/j.cnki.cjbhh.2017.09.024.Mao BH, Li J, Wang YX, et al. Small for gestational age in relation to maternal folic acid supplementation and dietary folate intake[J]. Chinese Journal of Birth Health & Heredity, 2017, 25(9): 62-64. DOI: 10.13404/j.cnki.cjbhh.2017.09.024. [3] 邵炎涛, 黄东萍, 刘顺, 等. 壮族地区孕前体质指数、孕期增重及孕期贫血对小于胎龄儿影响研究[J]. 中华疾病控制杂志, 2018, 22(7): 663-666. DOI: 10.16462/j.cnki.zhjbkz.2018.07.003.Zhao YT, Huang DP, Liu S, et al. Impact of maternal pre-pregnant body mass index, gestational weight gain and pregnant anemia on SGA in Zhuang Region[J]. Chin J Dis Control Prev, 2018, 22(7): 663-666. DOI: 10.16462/j.cnki.zhjbkz.2018.07.003. [4] Ricci E, Parazzini F, Chiaffarino F, et al. Pre-pregnancy body mass index, maternal weight gain during pregnancy and risk of small-for-gestational age birth: results from a case-control study in Italy[J]. J Matern Fetal Neonatal Med, 2010, 23(6): 501-505. DOI: 10.1016/j.preghy.2018.04.005. [5] 陈亚, 王剑, 倪亚莉, 等. 妊娠期合并疾病与小于胎龄儿的相关性分析[J]. 解放军预防医学杂志, 2016, 34(6): 876-878. DOI: 10.13704/j.cnki.jyyx.2016.06.030.Chen Y, Wang J, Ni YL, et al. Correlation between pregnancy complicated with diseases and small for gestational age status[J]. J Prev Med Chin PLA, 2016, 34(6): 876-878. DOI: 10.13704/j.cnki.jyyx.2016.06.030. [6] Copel JA, Bahtiyar MO. A practical approach to fetal growth restriction[J]. Obstet Gynecol, 2014, 123(5): 1057-1069. DOI: 10.1097/AOG.0000000000000402. [7] Guidelines IOM U, Rasmussen KM, Yaktine AL. Weight gain during pregnancy: reexamining the guidelines[M]. Washington, DC: National Academies Press, 2009: 2-3. [8] Jiang R, Tang W, Wu X, et al. A random forest approach to the detection of epistatic interactions in case-control studies[J]. BMC Bioinformatics, 2009, 10(Suppl 1): S65. DOI: 10.1186/1471-2105-10-S1-S65. [9] 丁海燕, 夏木斯叶·木依都力, 李敏超, 等. 舟山市2002-2015年出生体重变化与不良出生结局及影响因素分析[J]. 中华疾病控制杂志, 2018, 22(4): 380-385. DOI: 10.16462/j.cnki.zhjbkz.2018.04.014.Ding HY, XiaMuSiYe MYDL, Li MC, et al. Analysis of trends of birth weight, and incidence of adverse birth outcomes and relevant factors from 2002 to 2015[J]. Chin J Dis Control Prev, 2018, 22(4): 380-385. DOI: 10.16462/j.cnki.zhjbkz.2018.04.014. [10] Tuuli MG, Cahill A, Stamilio D, et al. Comparative efficiency of measures of early fetal growth restriction for predicting adverse perinatal outcomes[J]. Obstet Gynecol, 2011, 117(6): 1331-1340. DOI: 10.1097/AOG.0b013e31821ae239. [11] American college of obstetricians and gynecologists, gynecologists. ACOG Practice bulletin no. 134: fetal growth restriction[J]. Obstet Gynecol, 2013, 121(5): 1122-1133. DOI: 10.1097/01.AOG.0000429658.85846.f9. [12] Nardozza LM, Caetano AC, Zamarian AC, et al. Fetal growth restriction: current knowledge[J]. Arch Gynecol Obstet, 2017, 295(5): 1061-1077. DOI: 10.1007/s00404-017-4341-9(2017). [13] 高侃, 曹燚, 杨洁, 等. 胎儿生长受限危险因素的特征分析[J]. 中国超声医学杂志, 2016, 32(12): 1113-1115. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGCY201612020.htmGao K, Cao Y, Yang J, et al. Characteristics Analysis on Risk Factors of Fetal Growth Restriction[J]. Chinese Journal of Ultrasound in Medicine, 2016, 32(12): 1113-1115. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGCY201612020.htm [14] 钟鑫琪, 崔其亮. 早产儿和小于胎龄儿发生的危险因素的比较分析[J]. 中国当代儿科杂志, 2014, 16(12): 1202-1205. DOI: 10.7499/j.issn.1008-8830.2014.12.003.Zhong XQ, Cui QL. Comparative analysis of risk factors for preterm and small-for-gestational-age births[J]. Chin J Contemp Pediatr, 2014, 16(12): 1202-1205. DOI: 10.7499/j.issn.1008-8830.2014.12.003. [15] Thompson JM, Clark PM, Robinson E, et al. Risk factors for small-for-gestational-age babies: the auckland birthweight collaborative study[J]. J Paediatr Child Health, 2001, 37(4): 369-375. DOI: 10.1046/j.1440-1754.2001.00684.x. [16] 孔丽君, 周莉, 杨丽, 等. 足月单胎小于胎龄儿的围产结局及危险因素分析[J]. 现代医学, 2015, 43(10): 1230-1234. DOI: 10.3969/j.issn.1671-7562.2015.10.007.Kong LJ, Zhou L, Yang L, et al. Perinatal outcomes of small for gestational age and its risk factors[J]. Mod Med J, 2015, 43(10): 1230-1234. DOI: 10.3969/j.issn.1671-7562.2015.10.007. [17] Epifanio I. Intervention in prediction measure: a new approach to assessing variable importance for random forests[J]. BMC Bioinformatics, 2017, 18(1): 230. DOI: 10.1186/s12859-017-1650-8. -

 点击查看大图
点击查看大图

图(2) / 表(2)
计量
- 文章访问数: 289
- HTML全文浏览量: 163
- PDF下载量: 30
- 被引次数: 0