

Relationship between hyperuricemia and chronic kidney disease in adult residents of communities in the Songjiang district, Shanghai
-
摘要:
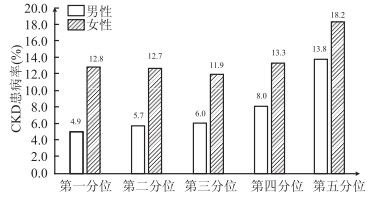
目的 分析社区居民高尿酸血症(hyperuricemia,HUA)及血清尿酸(serum uric acid,SUA)水平与慢性肾病(chronic kidney disease,CKD)的相关性。 方法 随机整群抽取上海市松江区新桥镇20~75岁的常住居民9 257名进行横断面调查,采用Logistic回归模型分析不同性别血清尿酸与慢性肾病的关系。 结果 不同性别分别依SUA水平将调查对象按五分位分为5组,男性CKD患病率依次为4.9%、5.7%、6.0%、8.0%和13.8%,女性CKD患病率依次为12.8%、12.7%、11.9%、13.3%和18.2%,且无论男女CKD患病率随着SUA水平升高均有增加趋势(均有P<0.05)。以SUA第一分位水平组为参照进行Logistic回归分析,男性第四、五分位水平组的调整OR值分别为2.12(95%CI:1.32~3.39)和3.84(95%CI:2.45~6.02),女性第五分位水平组的调整OR值为1.38(95%CI:1.05~1.80)。按SUA>420 μmol/L(男性)或>360 μmol/L(女性)标准定义HUA,在全体调查对象中,HUA与CKD明显相关(OR=2.03,95%CI:1.69~2.44,P<0.001),校正潜在混杂因素等后,两者仍独立相关(OR=2.04,95%CI:1.68~2.49,P<0.001),其中男性HUA患者CKD的患病风险是尿酸正常者的2.89倍(95%CI:2.12~3.94),女性是1.98倍(95%CI:1.51~2.60)。 结论 上海市松江区社区居民中,HUA可能是CKD的独立相关因素。 Abstract:Objective To explore the relationships between hyperuricemia (HUA), serum uric acid (SUA) level and the chronic kidney disease (CKD) in adult residents of communities. Methods A cross-sectional study was conducted in Xinqiao town of Songjiang district, Shanghai and a total of 9 527 residents aged 20-75 years were selected by random cluster sampling. Logistic regression models were used to evaluate the association between SUA and CKD. Results Subjects were divided into five groups according to the gender-specific quintiles of SUA. The CKD prevalence in serum uric acid quintiles of male were 4.9%, 5.7%, 6.0%, 8.0% and 13.8% respectively, while of female were 12.8%, 12.7%, 11.9%, 13.3% and 18.2% respectively, increasing along with the increase of SUA among both sexes (all P<0.05). Compared to the serum uric acid first quintile, the multivariate-adjusted odds for CKD in male of the fourth and fifth quintiles were 2.12 (95% CI: 1.32-3.39) and 3.84 (95% CI: 2.45-6.02), and the multivariate-adjusted odds for CKD in female of the fifth quintile was 1.38 (95% CI: 1.05-1.80). Hyperuricemia was defined by SUA>420 μmol/L(male) or >360 μmol/L(female). In the unadjusted model, HUA was significantly associated with CKD of all subjects (OR=2.03, 95% CI: 1.69-2.44, P<0.001), and the association was still significant (OR=2.04, 95% CI: 1.68-2.49, P<0.001) after adjustment for the potential confounders. The multivariate-adjusted odds of CKD associated with HUA was 2.89 (95% CI: 2.12-3.94, ) and 1.98 (95% CI: 1.51-2.60) for male and female, respectively. Conclusion Hyperuricemia was independently associated with the increased prevalence of CKD among community-based population living in the Songjiang district, Shanghai. -
Key words:
- Uric acid /
- Hyperuricemia /
- Chronic kidney disease /
- Cross-sectional study
-
表 1 不同SUA水平组的人口学及部分测量指标特征[M(P25, P75)]
Table 1. Demographics and partial measurement indicators of different SUA level groups[M(P25, P75)]
变量 第一分位水平组 第二分位水平组 第三分位水平组 第四分位水平组 第五分位水平组 F/H/χ2值 P值 男性 人数 676 683 678 665 668 年龄(岁) 59(52, 69) 56(48, 68) 54(45, 67) 54(41, 66) 53(41, 66) 101.82 <0.001 高血压史[n(%)] 226(33.4) 227(33.2) 229(33.8) 241(36.2) 298(44.6) 27.02 <0.001 糖尿病史[n(%)] 99(14.6) 65(9.5) 42(6.2) 44(6.6) 34(5.1) 51.76 <0.001 BMI(kg/m2) 23.87±3.13 24.09±3.09 24.61±3.19 25.06±3.29 25.97±3.33 46.06 <0.001 SBP(mmHg) 130.00(120.00, 146.00) 130.00(118.00, 144.50) 131.00(120.00, 146.00) 132.00(120.00, 144.00) 135.50(122.50, 148.00) 20.39 <0.001 DBP(mmHg) 78.00(71.50, 86.00) 78.00(71.50, 86.00) 80.00(72.00, 88.00) 82.00(74.00, 88.00) 82.00(75.50, 90.00) 69.85 <0.001 FPG(mmol/L) 4.58(4.21, 5.21) 4.51(4.21, 4.85) 4.50(4.19, 4.84) 4.49(4.18, 4.84) 4.48(4.21, 4.82) 15.67 0.003 HbA1c(%) 5.70(5.40, 6.20) 5.60(5.30, 5.90) 5.60(5.30, 5.90) 5.60(5.30, 6.00) 5.60(5.30, 5.90) 34.45 <0.001 TC(mmol/L) 4.63(4.09, 5.14) 4.64(4.06, 5.20) 4.61(4.09, 5.20) 4.66(4.11, 5.25) 4.77(4.27, 5.41) 21.06 <0.001 TG(mmol/L) 1.13(0.86, 1.62) 1.23(0.91, 1.71) 1.35(0.98, 1.95) 1.47(1.07, 2.19) 1.79(1.30, 2.74) 299.39 <0.001 LDL-C(mmol/L) 2.66(2.16, 3.12) 2.64(2.15, 3.12) 2.66(2.06, 3.10) 2.62(2.09, 3.11) 2.59(2.11, 3.14) 2.07 0.723 HDL-C(mmol/L) 1.38(1.16, 1.44) 1.35(1.13, 1.43) 1.27(1.08, 1.41) 1.26(1.05, 1.41) 1.20(0.99, 1.40) 123.07 <0.001 eGFR[mL·min-1· (1.73 m2)-1] 101.35±18.87 99.71±19.37 95.44±19.19 94.81±19.78 87.12±22.13 51.97 <0.001 女性 人数 970 989 946 975 957 年龄(岁) 52(43, 60) 52(42, 60) 53(45, 65) 54(45, 66) 56(49, 68) 69.00 <0.001 高血压史[n(%)] 173(17.8) 211(21.3) 228(24.1) 295(30.3) 402(42.0) 175.79 <0.001 糖尿病史[n(%)] 55(5.7) 66(6.7) 53(5.6) 59(6.1) 80(8.4) 8.20 0.085 BMI(kg/m2) 22.21(20.40, 24.26) 22.86(20.81, 24.96) 23.34(21.36, 25.78) 24.20(21.81, 26.52) 25.54(23.11, 28.08) 445.23 <0.001 SBP(mmHg) 126.00(112.00,143.00) 128.00(114.00, 144.00) 128.00(114.00, 144.00) 132.00(116.00, 148.00) 138.00(122.00, 153.00) 135.57 <0.001 DBP(mmHg) 74.00(68.00, 82.00) 74.00(68.00, 82.00) 74.00(68.00, 82.00) 76.00(70.00, 84.00) 78.00(72.00, 86.00) 102.05 <0.001 FPG(mmol/L) 4.50(4.19, 4.78) 4.45(4.17, 4.76) 4.48(4.19, 4.82) 4.51(4.21, 4.82) 4.56(4.21, 4.95) 25.42 <0.001 HbA1c(%) 5.60(5.30, 5.90) 5.60(5.30, 5.90) 5.60(5.40, 5.90) 5.70(5.40, 6.00) 5.70(5.40, 6.10) 86.72 <0.001 TC(mmol/L) 4.75(4.17, 5.40) 4.76(4.16, 5.41) 4.91(4.34, 5.47) 4.94(4.37, 5.63) 5.07(4.46, 5.77) 80.78 <0.001 TG(mmol/L) 1.03(0.78, 1.37) 1.13(0.85, 1.55) 1.23(0.90, 1.60) 1.34(0.98, 1.83) 1.57(1.14, 2.23) 432.21 <0.001 LDL-C(mmol/L) 2.63(2.10, 3.16) 2.60(2.12, 3.11) 2.78(2.27, 3.30) 2.78(2.27, 3.31) 2.84(2.29, 3.45) 51.94 <0.001 HDL-C(mmol/L) 1.62(1.42, 1.66) 1.58(1.36, 1.64) 1.56(1.31, 1.64) 1.48(1.26, 1.63) 1.40(1.19, 1.60) 271.60 <0.001 eGFR[mL·min-1· (1.73 m2)-1] 117.05±23.82 112.75±24.81 108.64±23.93 104.72±25.03 97.25±26.64 90.25 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 SUA五分位数组别与CKD患病的关系
Table 2. Relationship between quintiles of SUA and CKD
SUA水平组别 模型1 模型2 模型3 粗OR(95 % CI) 值 P值 粗OR(95 % CI) 值 P值 粗OR(95 % CI) 值 P值 男性 第一分位 1.00 1.00 1.00 第二分位 1.18(0.73~1.90) 0.496 1.31(0.81~2.13) 0.269 1.34(0.82~2.19) 0.240 第三分位 1.25(0.78~2.01) 0.346 1.56(0.96~2.52) 0.071 1.55(0.95~2.53) 0.080 第四分位 1.69(1.08~2.64) 0.022 2.13(1.35~3.38) 0.001 2.12(1.32~3.39) 0.002 第五分位 3.11(2.06~4.71) <0.001 3.98(2.59~6.12) <0.001 3.84(2.45~6.02) <0.001 女性 第一分位 1.00 1.00 1.00 第二分位 1.00(0.76~1.30) 0.977 1.00(0.76~1.30) 0.978 1.01(0.77~1.32) 0.967 第三分位 0.93(0.71~1.22) 0.577 0.90(0.68~1.18) 0.452 0.91(0.69~1.20) 0.508 第四分位 1.05(0.81~1.37) 0.719 1.00(0.76~1.30) 0.984 1.01(0.77~1.32) 0.971 第五分位 1.52(1.18~1.95) 0.001 1.36(1.05~1.76) 0.018 1.38(1.05~1.80) 0.021 注:模型1未调整;模型2调整年龄、高血压史、糖尿病史;模型3调整年龄、高血压史、糖尿病史、BMI、SBP、DBP、FPG、HbA1c、TC、TG、LDL-C、HDL-C。
下载: 导出CSV
表 3 HUA与CKD患病的关系
Table 3. Relationship between HUA and CKD
组别 检查人数 CKD[n(%)] χ2值 P值 粗OR (95% CI) 值 调整OR(95% CI) 值 全组 尿酸正常 7 326 758(10.3) 1.00 1.00 HUA 881 167(19.0) 58.28 <0.001 2.03(1.69~2.44) 2.04(1.68~2.49) 男性 尿酸正常 2 853 179(6.3) 1.00 1.00 HUA 517 79(15.3) 48.95 <0.001 2.69(2.03~3.58) 2.89(2.12~3.94) 女性 尿酸正常 4 473 579(12.9) 1.00 1.00 HUA 364 88(24.2) 34.78 <0.001 2.14(1.66~2.77) 1.98(1.51~2.60) 注:调整OR值为调整年龄、高血压史、糖尿病史、BMI、SBP、DBP、FPG、HbA1c、TC、TG、LDL-C、HDL-C。
下载: 导出CSV
-
[1] Coresh J. Update on the Burden of CKD[J]. Journal of the American Society of Nephrology, 2017, 28(4): 1020-1022. DOI: 10.1681/ASN.2016121374. [2] Gibson T. Hyperuricemia, gout and the kidney[J]. Curr Opin Rheumatol, 2012, 24(2): 127-131. DOI: 10.1097/BOR.0b013e32834f049f. [3] Hsu CY, Iribarren C, McCulloch CE, et al. Risk factors for end-stage renal disease: 25-year follow-up[J]. Arch Intern Med, 2009, 169(4): 342-350. DOI: 10.1001/archinternmed.2008.605. [4] Johnson RJ, Nakagawa T, Jalal D, et al. Uric acid and chronic kidney disease: which is chasing which?[J]. Nephrol Dial Transplant, 2013, 28(9): 2221-2228. DOI: 10.1093/ndt/gft029. [5] Feig DI. Uric acid: a novel mediator and marker of risk in chronic kidney disease?[J]. Curr Opin Nephrol Hypertens, 2009, 18(6): 526-530. DOI: 10.1097/MNH.0b013e328330d9d0. [6] Chou YC, Kuan JC, Yang T, et al. Elevated uric acid level as a significant predictor of chronic kidney disease: a cohort study with repeated measurements[J]. J Nephrol, 2015, 28(4): 457-462. DOI: 10.1007/s40620-014-0158-9. [7] Krishnan E, Akhras KS, Sharma H, et al. Serum urate and incidence of kidney disease among veterans with gout[J]. J Rheumatol, 2013, 40(7): 1166-1172. DOI: 10.3899/jrheum.121061. [8] Sedaghat S, Hoorn EJ, van Rooij FJ, et al. Serum uric acid and chronic kidney disease: the role of hypertension[J]. PLoS One, 2013, 8(11): e76827. DOI: 10.1371/journal.pone.0076827. [9] Mok Y, Lee SJ, Kim MS, et al. Serum uric acid and chronic kidney disease: the Severance cohort study[J]. Nephrol Dial Transplant, 2012, 27(5): 1831-1835. DOI: 10.1093/ndt/gfr530. [10] 周弋, 齐慧, 赵根明, 等. 上海市浦东新区居民高尿酸血症与慢性肾病相关性研究[J]. 中华流行病学杂志, 2012, 33(4): 351-355. DOI: 10.3760/cma.j.issn.0254-6450.2012.04.001.Zhou Y, Qi H, Zhao GM, et al. Relationship between hvperuricemia and chronic kidney disease in Pudong New Area of Shanghai[J]. Chin J Epidemiol, 2012, 33(4): 351-355. DOI: 10.3760/cma.j.issn.0254-6450.2012.04.001. [11] Yamada T, Fukatsu M, Suzuki S, et al. Elevated serum uric acid predicts chronic kidney disease[J]. Am J Med Sci, 2011, 342(6): 461-466. DOI: 10.1097/MAJ.0b013e318218bd89. [12] Wang S, Shu Z, Tao Q, et al. Uric acid and incident chronic kidney disease in a large health check-up population in Taiwan[J]. Nephrology(Carlton), 2011, 16(8): 767-776. DOI: 10.1111/j.1440-1797.2011.01513.x. [13] Bellomo G, Venanzi S, Verdura C, et al. Association of uric acid with change in kidney function in healthy normotensive individuals[J]. Am J Kidney Dis, 2010, 56(2): 264-272. DOI: 10.1053/j.ajkd.2010.01.019. [14] Kuriyama S, Maruyama Y, Nishio S, et al. Serum uric acid and the incidence of CKD and hypertension[J]. Clin Exp Nephrol, 2015, 19(6): 1127-1134. DOI: 10.1007/s10157-015-1120-4. [15] 邹贵勉, 黄江燕, 车文体, 等. 广西城市社区居民高尿酸血症流行病学调查及其与慢性肾脏病的关系[J]. 中华内分泌代谢杂志, 2011, 27(7): 561-565. DOI: 10.3760/cma.j.issn.1000-6699.2011.07.005.Zou GM, Huang JY, Che WT, et al. An epidemiological study on the prevalence of hyperuricemia and its relationship to chronic kidney disease in the urban community residents of Guangxi[J]. Chin J Endocrinol Metab, 2011, 27(7): 561-565. DOI: 10.3760/cma.j.issn.1000-6699.2011.07.005 [16] 全国eGFR课题协作组. MDRD方程在我国慢性肾脏病患者中的改良和评估[J]. 中华肾脏病杂志, 2006, 22(10): 589-595. DOI: 10.3760/j.issn:1001-7097.2006.10.002.Chinese eGFR Investigation Collaboration. Modification and evaluation of MDRD estimating equation for Chinese patients with chronic kidney disease[J]. Chin J Nephrol, 2006, 22(10): 589-595. DOI: 10.3760/j.issn:1001-7097.2006.10.002. [17] K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification[J]. Am J Kidney Dis, 2002, 39(2 Suppl 1): S1-S266 [18] 中华医学会内分泌学分会. 高尿酸血症和痛风治疗的中国专家共识[J]. 中华内分泌代谢杂志, 2013, 29(11): 913-920. DOI: 10.3760/cma.j.issn.1000-6699.2013.11.001.Endocrine committee of Chinese Medical Association. Chinese expert consensus on hyperuricemia and gout treatment[J]. Chin J Endocrinol Metab, 2013, 29(11): 913-920. DOI: 10.3760/cma.j.issn.1000-6699.2013.11.001. [19] Ren P, Gao M. Association Between Metabolic Syndrome and the Serum Uric Acid: a Cohort Study[J]. Clin Lab, 2018, 64(5): 719-726. DOI:10.7754/Clin.Lab, 2017.171037. [20] Abbasian M, Ebrahimi H, Delvarianzadeh M, et al. Association between serum uric acid (SUA) levels and metabolic syndrome (MetS) components in personnel of Shahroud University of Medical Sciences[J]. Diabetes Metab Syndr, 2016, 10(3): 132-136. DOI: 10.1016/j.dsx.2016.01.003. [21] Babio N, Martinez-Gonzalez MA, Estruch R, et al. Associations between serum uric acid concentrations and metabolic syndrome and its components in the PREDIMED study[J]. Nutr Metab Cardiovasc Dis, 2015, 25(23): 173-180. DOI: 10.1016/j.numecd.2014.10.006. -

 点击查看大图
点击查看大图
图(1) / 表(3)
计量
- 文章访问数: 252
- HTML全文浏览量: 230
- PDF下载量: 35
- 被引次数: 0