

Study on genotyping drug resistance of HIV/AIDS patients with antiviral failure from 2014 to 2016 in Yunnan Province
-
摘要:
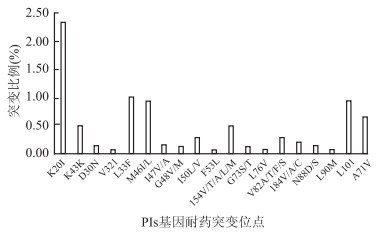
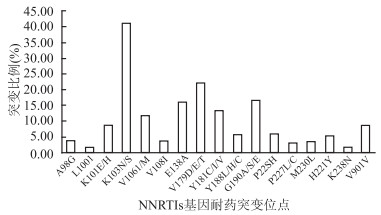
目的 调查云南省16个州市2014-2016年接受抗病毒治疗失败的感染人类免疫缺陷病毒/艾滋病免疫缺陷综合征(human immunodeficiency virus/acquired immune deficiency syndrome,HIV/AIDS)患者基因型耐药变异、耐药程度及突变位点分布情况。 方法 采用横断面调查方法,收集患者耐药相关流行病学信息。通过In-house方法,运用逆转录-聚合酶链式反应(reverse transcription-polymerase chain reaction,RT-PCR)扩增患者HIV-1 pol基因序列,测序后进行比对分析,阐明三类抗病毒药物耐药情况。 结果 2014-2016年全省发生耐药突变1 368(58.8%)例。粗略估计HIV-1总体耐药率为1.6%(1 368/84 146)。16个地市均有耐药毒株出现,总体耐药率以昭通市最高为4.5%,治疗失败人群耐药率最高为德宏,达到72.9%(100/145)。核苷类抑制剂(nucleoside reverse transcriptase inhibitors,NRTIs)、非核苷类抑制剂(non-nucleoside reverse transcriptase inhibitors,NNRTIs)以及蛋白酶抑制剂(protease inhibitor,PIs)的耐药率分别为51.1%(699/1 368)、91.2%(1 248/1 368)和9.6%(132/1 368);三类药物出现频率最高的突变位点依次为NRTIs-M184V(71.1%)、NNRTIs-K103N(43.7%)和PIs-K20I(24.2%)。 结论 目前云南省的HIV-1耐药呈现低流行水平,耐药率在各地市的分布存在一定差异,三类药物中以NNRTIs和NRTIs耐药为主,全省总体耐药情况与2008-2012年结果比较变化明显。我们应加强抗病毒治疗的管理和基因型耐药的检测,以降低耐药发生率,控制耐药毒株发生和传播。 -
关键词:
- 人类免疫缺陷病毒-1 /
- 高效联合抗逆转录病毒治疗 /
- 基因型耐药 /
- 突变位点
Abstract:Objective To investigate and analyze the prevalence, variation and mutations of genotyping drug resistance of human immunodeficiency virus/acquired immune deficiency syndrome(HIV/AIDS) patients with treatment failure from 16 prefectures in Yunnan Province from 2014 to 2016. Methods A cross-sectional study was conducted and epidemiological information collected from subject investigated. Reverse transcription-polymerase chain reaction(RT-PCR) was used to amplify HIV-1 pol gene fragments adopt In-house method, the alignment analysis was underway after sequencing, elucidated the resistant state of the three types of antiviral drugs. Results Based on the total patients treated from 2014 to 2016, 1 368 cases (58.8%) with drug-resistant mutations occurred all over province. A rough estimate of the overall resistance rate of HIV-1 was 1.6% (1 368/84 146). Drug-resistant strains were found in 16 cities. The highest overall drug resistant rate was 4.5% of Zhaotong, and among treatment failure population was Dehong's 72.9%(100/145). The mutations rates of nucleoside reverse transcriptase inhibitors(NRTIs), non-nucleoside reverse transcriptase inhibitors(NNRTIs) and protease inhibitors(PIs) in viral failure patients were 51.1% (699/1 368), 91.2% (1 248/1 368), 9.6%(132/1 368);The mutation sites with the highest frequency of the three kinds of drugs were NRTIs-M184V (71.1%), NNRTIs-K103N (43.7%), PIs-K20I (24.2%). Conclusions At present, HIV-1 drug resistance in Yunnan shows a low prevalence level, and there is a certain difference of resistant rate distribution in various cities. NNRTIs and NRTIs give priority to the drug resistance among the three kinds of drugs, the overall situation is significantly different from results of 2008-2012. We should strengthen the management of antiviral therapy and the detection of genotypic resistance, reduce the incidence of drug resistance, and control the occurrence and spread of drug-resistant strains. -
Key words:
- HIV-1 /
- Highly active antiretroviral theropy /
- Drug resistance /
- Mutation
-

图 1 云南省HIV/AIDS患者NNRTIs基因耐药突变位点比例
Figure 1. Proportion of mutations resistant to HIV-1 NNRTIs

图 2 云南省HIV/AIDS患者NRTIs基因耐药突变位点比例
Figure 2. Proportion of mutations resistant to HIV-1 NRTIs

图 3 云南省HIV/AIDS患者PIs基因耐药突变位点比例
Figure 3. Proportion of mutations resistant to HIV-1 PIs

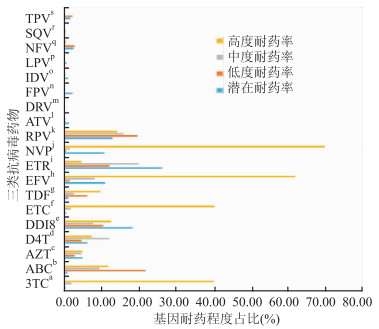
图 4 三类抗病毒治疗药物耐药程度分布
注:a拉米夫定(3TC);b阿巴卡韦(ABC);c齐多夫定(AZT);d司他夫定(d4T);e双脱氧肌苷(DDI);f恩曲他滨(FTC);g替诺福维(TDF);h依非维伦(FTC);i依曲韦林(ETR);j奈韦拉平(NVP);k利匹韦林(RPV);l阿扎那韦(ATV);m达芦那韦(DRV);n福沙那韦(FPV);o茚地那韦(IDV);p洛匹那韦(LPV);q奈非那韦(NFV);r沙奎那韦(SQV);s替拉那韦(TPV)。
Figure 4. Degrees of drug resistant to three kinds of antiviral drugs
表 1 云南省2014-2016年抗病毒失败患者人口学特征分布[n(%)]
Table 1. Demographic characteristics of patients with antiviral failure in Yunnan Province from 2014 to 2016[n(%)]
特征 扩增阳性数 耐药 敏感 χ2值 P值 性别 0.427 0.536 男 1 519 900(59.2) 619(40.8) 女 809 468(57.8) 341(42.2) 年龄(岁) 4.013 0.404 20~ 1 060 621(58.6) 439(41.4) 40~ 883 556(59.9) 372(40.1) 60~ 256 157(61.3) 99(38.7) ≥80 16 10(62.5) 6(37.5) 未知 36 0(0.0) 36(100.0) 传播途径 46.001 < 0.001 性接触 1 474 886(39.9) 588(60.1) 静脉药瘾 588 291(49.5) 297(50.5) 同性 35 27(77.1) 8(22.9) 母婴 34 30(88.2) 4(11.8) 其他 197 134(68.0) 63(32.0) 用药方案 26.137 < 0.001 3TCa+AZTb+NVPc 579 385(66.5) 194(33.5) 3TC+AZT+EFVd 672 387(57.6) 285(42.4) 3TC+TDFe+EFV 564 322(57.1) 242(42.9) 3TC+TDF+NVP 50 39(78.0) 11(22.0) 3TC+TDF+克力芝 221 116(52.5) 105(47.5) 3TC+AZT+克力芝 185 88(47.6) 97(52.4) 其他 57 31(54.4) 26(45.6) CD4+T淋巴细胞计数(个/μL) 156.517 < 0.001 ≤200 788 579(73.5) 209(26.5) 201~ 1 053 557(52.9) 496(47.1) 401~ 261 112(42.9) 149(57.1) 601~ 57 14(24.6) 43(75.4) ≥801 24 4(16.7) 20(83.3) 未知 145 102(70.3) 43(29.7) VL(copies/ml) 8.573 0.199 1 000~ 1 137 688(60.5) 449(39.5) 10 000~ 341 185(54.3) 156(45.7) 20 000~ 168 93(55.4) 75(44.6) 30 000~ 101 64(63.4) 37(36.6) 40 000~ 97 50(51.5) 47(48.5) 50 000~ 65 41(63.1) 24(36.9) ≥60 000 419 247(58.9) 172(41.1) 注:a拉米夫定;b齐多夫的;c奈韦拉平;d依非韦伦;e替诺福韦  下载: 导出CSV
下载: 导出CSV
表 2 云南省2014-2016年抗病毒治疗后耐药情况及三类药物耐药率[n(%)]
Table 2. State of drug resistance and incidence among three kinds of drugs from 2014 to 2016[n(%)]
耐药检测情况 年份 2014 2015 2016 年末累计治疗人数(例) 62 600 74 546 84 146 扩增阳性数(例) 612 809 907 耐药发生总数(例) 340 508 520 耐药发生数占扩增阳性比(%) 55.6 62.8 57.3 NRTIs 151(44.4) 261(51.4) 287(55.2) NNRTIs 303(89.1) 469(92.3) 476(91.5) PIs 33(9.7) 43(8.5) 56(10.8)
下载: 导出CSV
表 3 云南省2014-2016年各州市耐药检测与耐药率发生情况[n(%)]
Table 3. State of drug resistance and incidence among various prefectures in Yunnan Province from 2014 to 2016[n(%)]
地区 年末累计治疗(例) 扩增阳性数(例) 耐药发生数(例) 耐药发生占扩增阳性比例(%) 耐药率(%) NRTIs NNRTIs PIs 昆明 9 719 309 176 57.0 1.8 104(59.1) 158(89.8) 23(13.1) 德宏 9 882 59 43 72.9 0.4 19(44.2) 42(97.7) 3(7.0) 红河 16 050 546 299 54.8 1.9 163(54.5) 256(85.6) 29(9.7) 临沧 7 048 145 100 69.0 1.4 56(56.0) 94(94.0) 14(14.0) 保山 4 142 93 50 53.8 1.2 25(50.0) 48(96.0) 6(12.0) 楚雄 2 956 110 62 56.4 2.1 27(43.5) 56(90.3) 8(12.9) 大理 6 764 258 154 59.7 2.3 67(43.5) 145(94.4) 10(6.5) 怒江 633 38 24 63.2 3.8 17(70.8) 23(95.8) 2(8.3) 普洱 3 851 113 71 62.8 1.8 31(43.7) 66(93.0) 6(8.5) 曲靖 4 666 166 93 56.0 2.0 51(54.8) 88(94.6) 6(6.5) 文山 7 617 57 39 68.4 0.5 14(35.9) 37(94.9) 3(7.7) 版纳 1 803 58 36 62.1 2.0 25(69.4) 34(94.4) 6(16.7) 迪庆 184 3 3 100.0 1.6 2(66.7) 3(100.0) 0(0.0) 丽江 767 12 8 66.7 1.0 4(50.0) 8(100.0) 0(0.0) 昭通 3 112 236 141 59.7 4.5 61(43.3) 128(90.8) 12(8.5) 玉溪 3 024 99 56 56.6 1.9 26(46.4) 49(87.5) 4(7.1) 监狱 1 924 26 13 50.0 0.7 7(53.8) 13(100.0) 0(0.0) 总计 84 146 2 328 1 368 58.8 1.6 699(51.1) 1 248(91.2) 13(1.0)
下载: 导出CSV
表 4 HIV耐药突变可能影响因素的回归方程分析模型
Table 4. Regression equation analysis model for possible factors affecting HIV drug resistant mutation
模型中变量 β P值 OR(95 % CI)值 用药方案分别引进方程P值 CD4+T淋巴细胞计数 0.004 < 0.001 1.004(1.003~1.005) 用药方案 3TCa+AZTb+NVPc -0.399 0.194 0.671(0.367~1.225) < 0.001 3TC+AZT+EFVd -0.055 0.857 0.947(0.522~1.716) 0.649 3TC+TDFe +EFV -0.000 0.999 1.000(0.548~1.822) 0.381 3TC+TDF+NVP -1.080 0.025 0.340(0.132~0.872) 0.028 3TC+TDF+LPV/rf 0.263 0.421 1.301(0.685~2.469) 0.033 3TC+AZT+LPV/r 0.361 0.279 1.434(0.746~2.758) 0.006 常量 -1.396 < 0.001 0.248 注:a拉米夫定(3TC);b齐多夫定(AZT);c奈韦拉平(NVP);d依非韦伦(EFV);e替诺福韦(TDF);f洛匹那韦+利托那韦(LPV/r,克力芝)。
下载: 导出CSV
-
[1] Fauci AS. Twenty-five years of HIV/AIDS[J]. Science, 2006, 315(5786): 409. DOI:10. 1126/science.1131993. [2] Ho DD, Neumann AU, Perelson AS, et al. Rapid turnover of plasma virions and CD4 lymphocytes in HIV-1 infection[J]. Nature, 1995, 373(6510): 123-126. DOI: 10.1038/373123a0. [3] 周莹, 卢静, 张之, 等. 江苏省艾滋病一线药物抗病毒治疗失败病人的耐药特征及影响因素分析[J]. 中华疾病控制杂志, 2017, 21(12): 1191-1199. DOI: 10.16462/j.cnki.zhjbkz.2017.12.002.Zhou Y, Lu J, Zhang Z, et al. Risk factors associated with HIV drug resistance among ART virological failure patients taking first-line antiviral treatment from Jiangsu Province[J]. Chin J Dis Control Prev, 2017, 21(12): 1191-1199. DOI: 10.16462/j.cnki.zhjbkz.2017.12.002. [4] 梁欣, 彭晓霞. 中国HIV感染者和艾滋病患者抗逆转录病毒治疗后耐药情况的Meta分析[J]. 国际流行病学传染病学杂志, 2016, 43(3): 197-202. DOI: 10.3760/cma.j.issn.1673-4149.2016.03.012.Liang X, Peng XX. Meta-analysis on drug resistance of HIV infections and AIDS patients after antiretroviral therapy in China[J]. Inter J Epidemiol Infect Dis. 2016, 43(3): 197-202. DOI: 10.3760/cma.j.issn.1673-4149.2016.03.012. [5] 杨绍敏, 钟敏, 杨壁珲, 等. 云南省2008-2012年HIV-1耐药基因型检测情况[J]. 中国艾滋病性病. 2014, 20(1): 862-866. DOI: 10.13419/j.cnki.aids.2014.01.007.Yang SM, Zhong M, Yang BH, et al. Drug resistance detection of AIDS antiviral treatment in Yunnan from 2008 to 2012[J]. Chin J AIDS STD. 2014, 20(1): 862-866. DOI: 10.13419/j.cnki.aids.2014.01.007. [6] 钟敏, 杨壁珲, 杨绍敏. 云南地区123例艾滋病抗病毒治疗失败病人的HIV-1基因耐药突变位点分析[J]. 中华检验医学杂志, 2013, 36(1): 53-58. DOI: 10.3760/cma.j.issn.1009-9158.2013.01.014.Zhong M, Yang BH, Yang SM. Analysis of genotype resistance mutations sites among 123 antiretroviral-therapy failure in HIV/AIDS patients in Yunnan Province, China[J]. Chin J Lab Med, 2013, 36(1): 53-58. DOI: 10.3760/cma.j.issn.1009-9158.2013.01.014. [7] 楼金成, 李惠琴, 劳云飞, 等. 云南省成人AIDS病人抗病毒治疗的疗效分析[J]. 中国艾滋病性病, 2013, 19(8): 557-559. DOI:10.13419/j.cnki.aids, 2013.08.015.Lou JC, Li HQ, Lao YF, et al. Effectiveness analysis on antiretroviral therapy among HIV infected adults in Yunnan[J]. Chin J AIDS STD. 2013, 19(8): 557-559. DOI: 10.13419/j.cnki.aids.2013.08.015. [8] Sashi S. National anti-retroviral therapy guidelines[M]. Kathmandu: National Centre AIDS & STD Control. 2009: 15-21. [9] 左中宝, 邢辉. 抗病毒治疗患者HIV耐药发生的研究进展[J]. 传染病信息, 2015, 28(6): 348-351. DOI: 10.3969/j.issn.1007-8134.2015.06.004.Zuo ZB, Xing H. Research advances in HIV drug resistance among patients receiving antiretroviral treatment[J]. Infect Dis Info, 2015, 28(6): 348-351. DOI: 10.3969/j.issn.1007-8134.2015.06.004. [10] Wu J, Norris J, Liu HX, et al. The prevalence of HIV-1 drug resistance among treatment-failure individuals and treatment-naive individuals in China: a meta-analysis[J]. Biomed Environ Sci, 2014, 27(11): 858-871. DOI: 10.3967/bes2014.123. [11] 卢静, 周莹, 徐晓琴, 等. 江苏省抗病毒治疗失败HIV/AIDS患者耐药情况及基因型分析[J]. 江苏预防医学, 2016, 27(4): 388-391. DOI: 10.13668/j.issn.1006-9070.2016.04.002.Lu J, Zhou Y, Xu XQ, et al. Analysis of drug resistance and related genotypic mutations among HIV/AIDS patients who failed in antiretroviral therapy in Jiangsu Province[J]. Jiangsu J Prev Med, 2016, 27(4): 388-391. DOI: 10.13668/j.issn.1006-9070.2016.04.002. [12] 吴薇, 李娜, 刘昕亮, 等. 2014年乐山市HIV-1患者抗病毒治疗耐药性分析[J]. 预防医学情报杂志, 2017, 33(1): 25-29. https://www.cnki.com.cn/Article/CJFDTOTAL-YFYX201701007.htmWu W, Li N, Liu XL, et al. Analysis on drug resistance and subtype of HIV-1 patients receiving antiretroviral treatment in Leshan City, Sichuan Province[J]. J Prev Med Inf, 2017, 33(1): 25-29. https://www.cnki.com.cn/Article/CJFDTOTAL-YFYX201701007.htm [13] Hiwot HS, Michael RJ, Elliot R, et al. The HIV drug resistance report 2017[EB/OL]. (2017-09-23)[2019-02-13]. http://www.indiaenvironmentportal.org.in/files/file/HIV%20drug%20resistance%20report%202017.pdf. [14] Espindola MS, Lima LJ, Soares LS, et al. Dysregulated immune activation in second-line HAART HIV+ patients is similar to that of untreated patients[J]. PLoS One, 2015, 10(12): e0145261. DOI: 10.1371/journal.pone.0145261. [15] Iyidogan P, Anderson KS. Current perspectives on HIV-1 antiretroviral drug resistance[J]. viruses, 2014, 6(10): 4095-4139. DOI: 10.3390/v6104095. [16] 邵一鸣, 李敬云, 康来仪, 等. HIV耐药监测策略和检测技术[M]. 北京: 人民卫生出版社, 2010: 1-203.Shao YM, Li JY, Kang LY, et al. The strategy and methodology for HIV drug resistance surveillance and detection[M]. Beijing: People's Medical Publishing House, 2010: 1-203. -


 点击查看大图
点击查看大图
计量
- 文章访问数: 344
- HTML全文浏览量: 95
- PDF下载量: 25
- 被引次数: 0