

Analysis of gene mutation sites in patients with failed anti-HIV-1 treatment in Lincang City from 2011 to 2018
-
摘要:
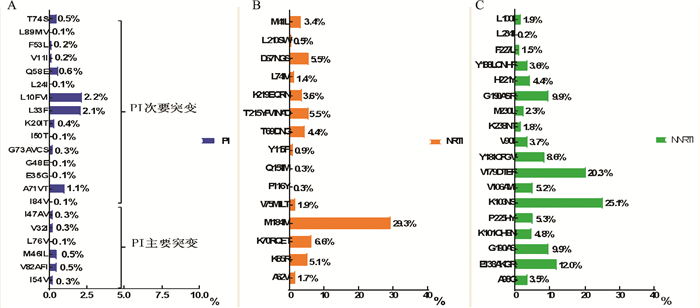
目的 了解云南省临沧市抗病毒治疗(antiretroviral therapy,ART)失败的人类免疫缺陷病毒(human immunodeficiency virus,HIV)感染者/艾滋病(aquired immunodeficiency syndrom,AIDS)患者的主要基因耐药突变位点及变化趋势。 方法 采用In-House方法,对2011-2018年临沧市ART失败的HIV/AIDS患者血浆样本进行Pol基因区扩增,目标序列经拼接整理提交至HIV耐药数据库,确定并分析HIV-1毒株亚型和耐药突变位点。 结果 950例ART失败的HIV/AIDS患者样本株以CRF08_BC为主占75.5%(717/950),总基因突变率为67.1%(637/950),以非核苷类反转录酶抑制剂(non-nucleoside reverse transcriptase inhibitors,NNRTIs)为主,占62.4%(593/950);其次是核苷类反转录酶抑制剂(nucleoside reverse transcriptase inhibitors,NRTIs)为34.7%(330/950);蛋白酶抑制剂(protease inhibitors,PIs)为7.5%(71/950)。累计检出耐药相关突变位点NRTIs类15种,主要为M184V(29.3%),在AZT/D4T+3TC+NVP方案中检出最多;NNRTIs类17种,主要为K103N/S(25.1%),在AZT/TDF+3TC+EFV方案中检出最多;PIs类22种,主要为次要位点L10F/V/I(2.2%),L33F(2.1%)。该地NRTIs类居前三位的突变位点由T69D/N/G,M184I/V和D67N/G/S变为M184I/V,K70R/Q/E/T和T215Y/F/V/I/N/A/D;NNRTIs类由V179D/T/E/F,E138A/K/G/R和Y181C/F/G/V变为K103N/S,E138A/K/G/R和V179D/T/E/F;PIs类突变位点变化不大。 结论 以PIs类为主的二线方案是目前免费ART较好的选择,掌握不同基因突变位点的耐药规律有利于一线药物间的换药配伍,从而延迟二线药物的使用。 Abstract:Objective To understand the major genotype-resistant mutation sites and change trends of HIV/AIDS patients with failure of antiviral therapy (ART) in Lincang City, Yunnan Province. Methods The In-House method was used to amplify the Pol gene region in the plasma samples of HIV/AIDS patients with failure of ART in Lincang City from 2011 to 2018. The target sequence was spliced and submitted to the HIV resistance database to identify and analyze the HIV-1 subtypes and resistant mutation sites. Results The 950 strains of HIV/AIDS patients with antiviral failure were mainly CRF08_BC, accounting for 75.5% (717/950), and the total gene mutation rate was 67.1% (637/950), which was dominated by non-nucleoside reverse transcriptase inhibitors (NNRTIs), accounting for 62.4% (593/950); followed by nucleoside reverse transcriptase inhibitors (NRTIs), accounting for 34.7% (330/950); protease inhibitors (PIs) was 7.5% (71/950). A total of 15 NRTIs of resistance-related mutation sites were detected, mainly M184V (29.3%) which was detected mostly in AZT/D4T+3TC+NVP programs; including 17 kinds of NNRTIs, mainly was K103N/S (25.1%), the most detected in AZT/TDF+3TC+EFV programs. There were 22 kinds of PIs, mainly secondary sites were L10F/V/I (2.2%) and L33F (2.1%). The top three NRTIs mutation sites in the area were changed from T69D/N/G, M184I/V and D67N/G/S to M184I/V, K70R/Q/E/T and T215Y/F/V/I/N/A/D. NNRTIs mutation sites were changed from V179D/T/E/F, E138A/K/G/R and Y181C/F/G/V to K103N/S, E138A/K/G/R and V179D/T/E/F. The mutation sites of the first three PIs did not change much. Conclusions The second-line regimen based on PIs is a better choice in free antiviral treatments. Mastering the drug resistance of different gene mutations is beneficial to the compatibility of first-line drugs, thus delaying the use of second-line drugs. -
Key words:
- HIV/AIDS /
- Antiviral failure /
- Mutation site /
- Drug resistance trend
-

图 1 2011-2018年临沧地区HIV-1抗病毒失败患者样本各年亚型分布
Figure 1. Distribution of subtypes of HIV-1 antiviral failure patients in Lincang area from 2011 to 2018

图 2 2011-2018年临沧市HIV-1抗病毒失败患者耐药和耐药相关突变情况
Figure 2. Drug-resistant and drug-resistant mutations in HIV-1 antiviral failure patients in Lincang City from 2011 to 2018

图 3 2011-2018年云南省临沧市HIV-1抗病毒失败患者耐药相关的突变位点
Figure 3. Drug-related mutation sites in HIV-1 antiviral failure patients in Lincang City, Yunnan Province from 2011 to 2018

图 4 2011-2018年云南省临沧市HIV-1抗病毒失败患者各年NRTIs和NNRTIs耐药相关突变位点频率变化趋势
Figure 4. The trends of NRTIs and NNRTIs resistance-related mutations in HIV-1 patients with HIV-1 failure in Lincang City, Yunnan Province from 2011 to 2018

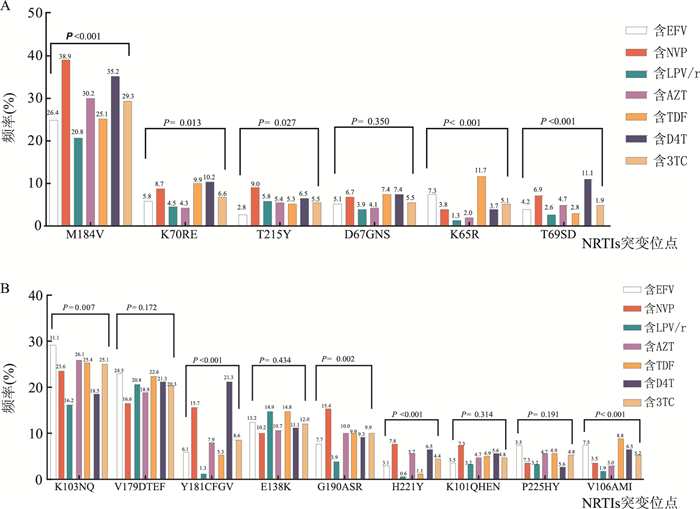
图 5 不同治疗药物的抗HIV-1治疗失败患者主要突变位点检出情况
Figure 5. Detection of major mutation sites in patients with failed HIV-1 treatment for different treatments
表 1 接受不同治疗方案的抗HIV-1治疗失败患者主要突变位点检出情况
Table 1. Detection of major mutation sites in patients with failed HIV-1 treatment receiving different treatment regimens
突变位点 AZT+3TC+
NVP(n=248)AZT+3TC+
EFV(n=240)TDF+3TC+
NVP(n=9)TDF+3TC+
EFV(n=191)AZT+3TC+
LPV/r(n=71)TDF+3TC+
LPV/r(n=83)D4T+3TC+
NVP(n=87)D4T+3TC+
EFV(n=21)NRTIs M184IV 97(39.1) 54(22.5) 2(22.2) 55(28.8) 18(25.4) 14(16.9) 35(40.2) 3(14.3) K70RE 17(6.9) 6(2.5) 2(22.2) 20(10.5) 1(1.4) 6(7.2) 11(12.6) 0(0.0) T215Y 25(10.1) 4(1.7) 0(0.0) 7(3.7) 1(1.4) 8(9.6) 6(6.9) 1(4.8) D67GNS 15(6.0) 7(2.9) 1(11.1) 15(7.9) 1(1.4) 5(6.0) 7(8.0) 1(4.8) K65R 10(4.0) 0(0.0) 0(0.0) 32(16.8) 1(1.4) 1(1.2) 3(3.4) 1(4.8) T69SD 12(4.8) 13(5.4) 0(0.0) 5(2.6) 1(1.4) 3(3.6) 12(13.8) 0(0.0) NNRTIs K103NQ 64(25.8) 69(28.8) 1(11.1) 59(30.9) 13(18.3) 12(14.5) 16(18.4) 4(19.0) V179DTEF 38(15.3) 53(22.1) 1(11.1) 46(24.1) 15(21.1) 17(20.5) 18(20.7) 5(23.8) E138K 26(10.5) 25(10.4) 0(0.0) 28(14.7) 9(12.7) 14(16.9) 9(10.3) 3(14.3) G190ASR 42(16.9) 13(5.4) 1(11.1) 22(11.5) 1(1.4) 5(6.0) 10(11.5) 0(0.0) Y181CFGV 31(12.5) 11(4.6) 1(11.1) 14(7.3) 2(2.8) 0(0.0) 22(25.3) 1(4.8) H221Y 20(8.1) 11(4.6) 0(0.0) 3(1.6) 1(1.4) 0(0.0) 7(8.0) 0(0.0) P225HY 10(4.0) 18(7.5) 0(0.0) 14(7.3) 3(4.2) 2(2.4) 2(2.3) 1(4.8) V106AMI 4(1.6) 12(5.0) 2(22.2) 21(11.0) 1(1.4) 2(2.4) 6(6.9) 1(4.8) K101QHEN 19(7.7) 6(2.5) 1(11.1) 9(4.7) 1(1.4) 4(4.8) 5(5.7) 1(4.8)  下载: 导出CSV
下载: 导出CSV
-
[1] Hu TS, Zhang HL, Feng Y, et al. Epidemiological and molecular characteristics of emergent dengue virus in Yunnan Province near the China-Myanmar-Laos border, 2013-2015[J]. BMC Infect Dis, 2017, 17: 331. DOI: 10.1186/s12879-017-2401-1. [2] 苏俊琪. 抗病毒治疗失败病人的耐药特征及HIV-1耐药准种与毒株适应性的关系[D]. 北京: 中国疾病预防控制中心, 2011.Su JQ. The drug resistance characteristics of patients with antiviral treatment failure and the relationship between HIV-1 resistance quasispecies and strain adaptability[D]. Beijing: China Center for Disease Control and Prevention, 2011. [3] Abram ME, Ferris AL, Das K, et al. Mutations in HIV-1 reverse transcriptase affect the errors made in a single cycle of viral replication[J]. Hughes J Virol, 2014, 88(13): 7589-7601. DOI: 10.1128/JVI.00302-14. [4] Xiao PP, Li JJ, Fu GF, et al. Geographic distribution and temporal trends of HIV-1 subtypes through heterosexual transmission in China: A systematic review and meta-analysis[J]. Int J Environ Res Public Health, 2017, 14(7): 830. DOI: 10.3390/ijerph14070830. [5] Chen M, Yang L, Ma YL, et al. Emerging variability in HIV-1 genetics among recently infected individuals in Yunnan, China[J]. PLoS One, 2013, 8(3): e60101. DOI: 10.1371/journal.pone.0060101. [6] 刘家法, 张米, 李健健, 等. 含洛匹那韦/利托那韦二线方案抗HIV病毒治疗失败基因型耐药情况分析[J]. 重庆医学, 2018, 47(34): 4399-4402. DOI: 10.3969/j.issn.1671-8348.2018.34.019.Liu JF, Zhang M, Li JJ, et al. Analysis of genotypic resistance of anti-HIV virus treatment failure with lopinavir/ritonavir second-line regimen[J]. Chongqing Yixue, 2018, 47(34): 4399-4402. DOI: 10.3969/j.issn.1671-8348.2018.34.019. [7] 陈荣华, 李勤光, 卓传尚, 等. 福建省HIV-1毒株亚型分布分析[J]. 中国卫生标准管理, 2019, 10(7): 4-6.Chen RH, Li QG, Zhuo CS, et al. Distribution of HIV-1 strain subtypes in Fujian Province[J]. Chinese Health Standards Management, 2019, 10(7): 4-6. [8] 王凤英, 顾建华, 金涛, 等. 新疆第四次HIV分子流行病学调查分析[J]. 疾病预防控制通报, 2018, 33(6): 1-2, 27. DOI: 10.13215/j.cnki.jbyfkztb.1808020.Wang FY, Gu JH, Jin T, et al. The fourth epidemiological investigation of HIV in Xinjiang[J]. Bull Dis Control Prev, 2018, 33(6): 1-2, 27. DOI: 10.13215/j.cnki.jbyfkztb.1808020. [9] 刘佳, 闫江舟, 胡凯, 等. 河南省2014-2016年不同城市新确证HIV感染者的亚型分布和耐药传播情况分析[J]. 中国皮肤性病学杂志, 2019, 33(4): 437-441. DOI: 10.13735/j.cjdv.1001-7089.201805160.Liu J, Yan JZ, Hu K, et al. Analysis of subtype distribution and drug resistance transmission of newly confirmed HIV-infected people in different cities in Henan Province from 2014 to 2016[J]. Chin J Derm Venereolo, 2019, 33(4): 437-441. DOI: 10.13735/j.cjdv.1001-7089.201805160. [10] 舒远路, 杨翠先, 张米, 等. 云南省HIV-1主要流行亚型毒株的耐药突变分析[J]. 中国艾滋病性病, 2018, 24(11): 1080-1084, 1114. DOI: 10.13419/j.cnki.aids.2018.11.03.Shu YL, Yang CX, Zhang M, et al. Analysis of drug resistance mutations of HIV-1 major subtype strains in Yunnan Province[J]. China AIDS and STD, 2018, 24(11): 1080-1084, 1114. DOI: 10.13419/j.cnki.aids.2018.11.03. [11] 焦丽燕, 李敬云. HIV-1耐药突变及突变型[J]. 中华医学杂志, 2009, (13): 931-936. DOI: 10.3760/cma.j.issn.0376-2491.2009.13.018.Jiao LY, Li JY. HIV-1 drug resistance mutations and mutations[J]. Chinese Journal of Medicine, 2009, (13): 931-936. DOI: 10.3760/cma.j.issn.0376-2491.2009.13.018. [12] 林兆森, 王卫军. HIV-1耐药性相关研究进展[J]. 微生物学免疫学进展, 2018, 46(4): 76-80. DOI: 10.13309/j.cnki.pmi.2018.04.014.Lin ZS, Wang WJ. Research progress on HIV-1 drug resistance[J]. Pro in Microbiol Immunol, 2018, 46(4): 76-80. DOI: 10.13309/j.cnki.pmi.2018.04.014. [13] 李彦媚, 赵红心, 周海卫, 等. AIDS患者高效一线抗逆转录病毒治疗失败后HIV耐药基因型分析[J]. 中华实验和临床感染病杂志, 2013, 7(1): 68-72. DOI: 10.3877/cma.j.issn.1674-1358.2013.01.018.Li YM, Zhao HX, Zhou HW, et al. Analysis of HIV drug resistance genotypes in patients with AIDS after high-efficiency first-line antiretroviral therapy failure[J]. Chin J Exp Clin Infect Dis, 2013, 7(1): 68-72. DOI: 10.3877/cma.j.issn.1674-1358.2013.01.018. [14] 邵一鸣, 李敬云, 康来仪, 等. HIV耐药监测策略和检测技术[M]. 北京: 人民卫生出版社, 2010: 45-53.Shao YM, Li JY, Kang LY, et al. HIV resistance monitoring strategy and detection technology[M]. Beijing: People's Medical Publishing House, 2010: 45-53. [15] 吴欣华, 杨兰辉, 霍松, 等. 红河州HAART的HIV/AIDS病人的耐药性及其影响因素[J]. 中国艾滋病性病, 2014, 20(10): 730-733, 741. DOI: 10.13419/J.cnki.aids.2014.10.037.Wu XH, Yang LH, Huo S, et al. Drug resistance and its influencing factors of HIV/AIDS patients in HAART of Honghe Prefecture[J]. Chin J AIDS STD, 2014, 20(10): 730-733, 741. DOI: 10.13419/J.cnki.aids.2014.10.037. [16] Scherrer AU, von Wyl V, Joos B, et al. Predictors for the emergence of the 2 multi-nucleoside/nucleotide resistance mutations 69 insertion and Q151M and their impact on clinical outcome in the Swiss HIV Cohort Study. [J]. J Infect Dis, 2011, 203: 791-797. DOI: 10.1093/infdis/jiq130. [17] Gupta RK, Gregson J, Parkin N, et al. HIV-1 drug resistance before initiationor re-initiation of first-line an-Titrotroviral therapy in low-incomeand middle-income countries: a Systemive review and meta-regression analysis[J]. Lancet Infect Dis, 2018, 18(3): 346-355. DOI: 10.1016/S1473-3099(17)30702-8. [18] Parkin NT, Gupta S, Chappey C, et al. The K101P and K103R/V179D mutations in human immunodeficiency virus type 1 reverse transcriptase confer resistance to nonnucleoside reverse transcriptase inhibitors[J]. Antimicrob Agents Chemother, 2006, 50(1): 351-354. DOI: 10.1128/AAC.50.1.351-354.2006. [19] Li HP, Zhong M, Guo W, et al. Prevalence and mutation paterns of HIV drug resistance from 2010 to 2011 among ART-failure individuals in the Yunnan Province, China[J]. PLoS One, 2013, 8(8): e72630. DOI: 10.1371/journal.pone.0072630. -



 点击查看大图
点击查看大图

计量
- 文章访问数: 520
- HTML全文浏览量: 290
- PDF下载量: 68
- 被引次数: 0