

Service demand and capacity of HIV prevention of mother-to-child transmission in Guangdong
-
摘要:
目的 分析广东省各地预防艾滋病母婴传播(mother-to-chlid transmission,MTCT)的服务需求与能力,了解工作的薄弱地区和环节。 方法 收集2014年-2017年广东省感染人类免疫缺陷病毒(human acquired immunodeficiency virus,HIV)的孕产妇及暴露婴儿的服务需求及干预情况,使用SPSS 21.0软件分析各地服务需求与能力差异,以及各地助产机构和母婴保健人员数量与HIV的MTCT之间相关性。 结果 感染HIV孕产妇文化程度不高,以初中为主(54.49%);各地感染HIV的孕产妇服务需求不同,珠三角区外来少数民族(12.96%)、山区非本地居住(43.75%)、东翼感染途径不详(77.78%)孕产妇占比高;各地服务能力不同,山区和东翼孕产妇多产时/产后确诊(占比41.67%和44.44%)、治疗晚(山区和东翼超过36周治疗或未治疗占比43.75%和55.56%)、孕产妇和婴儿未治疗比例高(山区和东翼为2.08%和33.33%),且东翼母乳喂养比例高(11.11%);东翼助产服务机构和母婴保健服务人员数量少,覆盖面小;各地助产机构和母婴保健人员数量与MTCT均无相关性(均有P>0.05)。 结论 山区和东翼是广东省预防HIV的MTCT工作薄弱地区,检测晚、干预不规范、信息质量低是薄弱环节。有针对地消除服务能力的地区差异,是实现广东省消除HIV的MTCT目标的关键。 Abstract:Objective To analyze the service demand and capacity for preventing mother-to-child transmission(MTCT) of acquired immune deficiency syndrome in Guangdong, as well as to find the weakness in the work. Methods The relevant data of service demands and intervention capacity of human acquired immunodeficiency virus(HIV)-infected maternal and their babies from 2014 to 2017 was collected, and SPSS 21.0 software was employed to analyze the differences among the pearl river delta area, western area, mountainous area and eastern area, and to explore the correlation between regional midwifery institutions or personnel numbers and the rate of HIV MTCT. Results The education of HIV-infected maternal wasn't high, generally, mainly in middle school (54.49%). The service demand of HIV-infected maternal was different in each area. The ethnic minorities outside the pearl river delta region (12.96%) and non-local living maternal in mountainous area (43.75%) were high. The proportion of maternal in the eastern area who didn't know the route of HIV infection was also high (77.78%). The service capacity varies in each area, and the proportion (mountainous area: 41.67%, eastern area: 44.44%) of the confirmation time in intrapartum/postpartum was high among those from the mountains and eastern areas, which lead to poor intervention (the proportions of starting to antiretroviral treatment time later than 36 weeks or untreated in mountainous and eastern areas were 43.75% and 55.56%, respectively), as well as a high proportion of untreated maternal and exposed-infant (mountainous area: 2.08%, eastern area: 33.33%), and a higher percentage (11.11%) of breastfeeding in eastern area. There was no significant correlation between the number of midwifery institutions or healthcare personnel and the rate of HIV MTCT in different regions. Conclusions The mountainous and eastern areas are the weak of HIV MTCT in Guangdong Province, and later detection, less-standard intervention, and lower quality of information management are the weak steps in those areas. Targeted measures should be urgently developed to strengthen the training of the key areas to eliminate the regional differences of service capacity, which is essential to achieve the elimination of HIV MTCT in Guangdong. -
Key words:
- HIV /
- Mother-to-child transmission /
- Midwifery institutions /
- Service demand /
- Service capacity
-

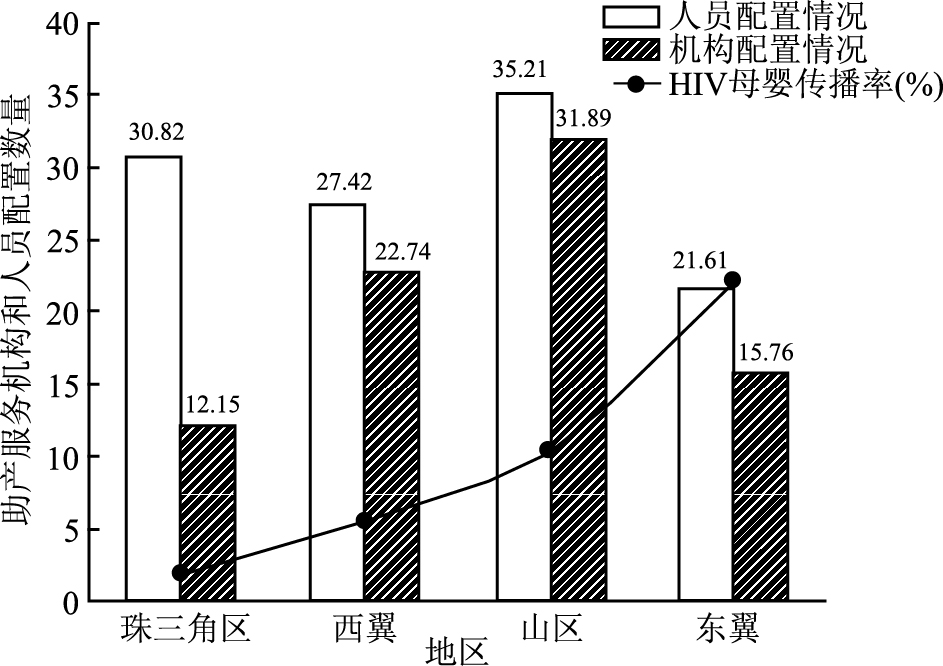
图 1 广东省各地区助产服务机构和人员配置数量与HIV母婴传播情况分析
Figure 1. Analysis of regional midwifery institution and personnel allocation numbers with the rate of HIV MTCT in Guangdong Province
表 1 广东省各地区感染HIV孕产妇和暴露婴儿的服务需求情况分析[n(%)]
Table 1. Analysis of service demand of HIV-infected maternal and exposed infants in Guangdong[n(%)]
特征变量 合计 分布地区 χ2/F值 P值 珠三角区(n=216) 西翼(n=72) 山区(n= 48) 东翼(n=9) 孕产妇 孕产妇年龄(岁,x±s) 29.32±5.55 29.28±5.69 29.54±5.33 29.88±5.48 25.44±3.13 1.67 0.173 年龄组(岁) 4.96 0.548 < 20 11 5(2.31) 4(5.56) 2(4.17) 0(0.00) 20~ 269 169(78.24) 53(73.61) 38(79.17) 9(100.00) ≥35 65 42(19.44) 15(20.83) 8(16.67) 0(0.00) 民族 4.66 0.014 汉族 312 188(87.04) 71(98.61) 44(91.67) 9(100.00) 其他 33 28(12.96) 1(1.39) 4(8.33) 0(0.00) 本地居住 8.60 0.034 是 251 161(74.54) 56(76.39) 27(56.25) 8(88.89) 否 94 55(25.46) 17(23.61) 21(43.75) 1(11.11) 文化程度 18.89 0.090 小学及以下 43 26(12.04) 8(11.11) 7(14.58) 2(22.22) 初中 188 105(48.61) 45(62.50) 32(66.67) 6(66.67) 高中 67 49(22.69) 13(18.06) 5(10.42) 0(0.00) 大学及以上 31 27(12.50) 2(2.78) 2(4.17) 0(0.00) 不详 16 9(4.17) 4(5.56) 2(4.17) 1(11.11) 可能的感染途径 16.58 0.036 性传播 200 137(63.43) 40(55.56) 21(43.75) 2(22.22) 血液传播 11 7(3.24) 1(1.39) 3(6.25) 0(0.00) 母婴传播 2 1(0.46) 1(1.39) 0(0.00) 0(0.00) 不详/其他 132 71(32.87) 30(41.67) 24(50.00) 7(77.78) 职业 26.87 0.008 家庭主妇/无业 190 118(54.63) 38(52.78) 30(62.50) 4(44.44) 工人 37 26(12.04) 5(6.94) 5(10.42) 1(11.11) 农民 47 17(7.87) 20(27.78) 8(16.67) 2(22.22) 商业服务 20 16(7.41) 3(4.17) 1(2.08) 0(0.00) 其他 51 39(18.06) 6(8.33) 4(8.33) 2(22.22) 婚姻状况 4.67 0.867 初婚 237 145(67.13) 51(70.83) 34(70.83) 7(77.78) 再婚 53 31(14.35) 13(18.06) 8(16.67) 1(11.11) 未婚/同居 50 37(17.13) 7(9.72) 5(10.42) 1(11.11) 离婚/丧偶 5 3(1.39) 1(1.39) 1(2.08) 0(0.00) 孕次a 15.69 0.011 1 80 55(25.82) 12(16.67) 7(14.58) 6(66.67) 2~ 196 119(55.87) 48(66.67) 26(54.17) 3(33.33) >3 66 39(18.31) 12(16.67) 15(31.25) 0(0.00) 产次 34.83 < 0.001 0 131 105(48.61) 14(19.44) 8(16.67) 4(44.44) 1~ 188 101(46.76) 49(68.06) 33(68.75) 5(55.56) >2 26 10(4.63) 9(12.50) 7(14.58) 0(0.00) 孕产期异常情况 1.66 0.642 无 269 171(79.17) 57(79.17) 34(70.83) 7(77.78) 有 76 45(20.83) 15(20.83) 14(29.17) 2(22.22) 分娩机构 15.95 0.033 地市级以上 183 126(58.33) 30(41.67) 25(52.08) 2(22.22) 县/区级 119 62(28.70) 33(45.83) 19(39.58) 5(55.56) 街道/乡镇级 37 25(11.57) 8(11.11) 2(4.17) 2(22.22) 其他(kg, x±s) 6 3(1.39) 1(1.39) 2(4.17) 0(0.00) 儿童 出生体重(kg, x±s) 2.97±0.49 3.02±0.49 2.88±0.52 2.93±0.43 2.86±0.42 1.83 0.142 出生身长(cm, x±s) 48.98±2.03 49.03±1.98 49.25±1.55 48.25±2.78 49.56±1.24 2.81 0.039 性别 7.09 0.068 男 179 115(53.24) 32(44.44) 30(62.50) 2(22.22) 女 166 101(46.76) 40(55.56) 18(37.50) 7(77.78) 早诊采血机构 54.39 < 0.001 地市级以上 167 115(53.24) 25(34.72) 27(56.25) 0(0.00) 县/区级 142 65(30.09) 47(65.28) 21(43.75) 9(100.00) 街道/乡镇级和其他 36 36(16.67) 0(0.00) 0(0.00) 0(0.00) 注:a孕次信息缺失3人。  下载: 导出CSV
下载: 导出CSV
表 2 广东省各地区预防HIV母婴传播工作服务能力分析[n(%)]
Table 2. Analysis of service capacity of PMTCT program in Guangdong[n(%)]
特征变量 合计 分布地区 χ2/t值 P值 珠三角区(n=216) 西翼(n=72) 山区(n= 48) 东翼(n=9) 机构分类 220.91 < 0.001 地市级以上 122 65(8.70) 19(5.21) 23(4.29) 15(5.49) 县/区级 329 146(19.54) 47(12.88) 84(15.67) 52(19.05) 街道/乡镇级 1 174 326(43.64) 260(71.23) 410(76.49) 178(65.20) 其他 296 210(28.11) 39(10.69) 19(3.55) 28(10.26) 检测 确认感染时期 24.81 < 0.001 孕前 103 71(32.87) 18(25.00) 13(27.08) 1(11.11) 孕期 172 117(54.17) 36(50.00) 15(31.25) 4(44.44) 产时/产后 70 28(12.96) 18(25.00) 20(41.67) 4(44.44) 性伴感染状态 7.50 0.251 阴性 127 89(41.20) 18(25.00) 18(37.50) 2(22.22) 阳性 82 49(22.69) 19(26.39) 12(25.00) 2(22.22) 不详 136 78(36.11) 35(48.61) 18(37.50) 5(55.56) 治疗 孕产妇抗病毒治疗 22.64 < 0.001 否 46 18(8.33) 10(13.89) 14(29.17) 4(44.44) 是 299 198(91.67) 62(86.11) 34(70.83) 5(55.56) 孕产妇抗病毒治疗时期(周) 28.76 < 0.001 < 13 116 81(37.50) 26(36.11) 8(16.67) 1(11.11) 13~ 122 84(38.89) 20(27.78) 17(35.42) 1(11.11) 28~ 18 10(4.63) 4(5.56) 2(4.17) 2(22.22) ≥36或未治疗 89 41(18.98) 22(30.56) 21(43.75) 5(55.56) 婴儿抗病毒治疗 21.87 < 0.001 否 7 1(0.46) 0(0.00) 3(6.25) 3(33.33) 是 338 215(99.54) 72(100.00) 45(93.75) 6(66.67) 母子抗病毒治疗 36.16 < 0.001 均治疗 297 198(91.67) 66(86.11) 32(66.67) 5(55.56) 仅一方治疗 43 17(7.87) 10(13.89) 15(31.25) 1(11.11) 均未治疗 5 1(0.46) 0(0.00) 1(2.08) 3(33.33) 安全助产和喂养 分娩方式 30.06 < 0.001 阴道产 176 87(40.28) 50(69.44) 30(62.50) 9(100.00) 择期剖宫产 101 77(35.65) 12(16.67) 12(25.00) 0(0.00) 急诊剖宫产 68 52(24.07) 10(13.89) 6(12.50) 0(0.00) 是否产科操作 8.25 0.040 否 293 190(87.96) 55(76.39) 42(87.50) 6(66.67) 是 52 26(12.04) 17(23.61) 6(12.50) 3(33.33) 喂养方式 31.54 < 0.001 母乳喂养 4 2(0.93) 0(0.00) 1(2.08) 1(11.11) 人工喂养 261 179(82.87) 41(56.94) 34(70.83) 7(77.78) 不详 80 35(16.20) 31(43.06) 13(27.08) 1(11.11)
下载: 导出CSV
-
[1] Diallo K, Kim AA, Lecher S, et al. Early diagnosis of HIV infection in infants-one caribbean and six sub-saharan african countries, 2011-2015[J]. MMWR Morb Mortal Wkly Rep, 2016, 65(46): 1285-1290. DOI: 10.15585/mmwr.mm6546a2. [2] World Health Organization. Preventing mother-to-child transmission (MTCT) of HIV[R]. Geneva: World Health Orgnization, 2012. [3] The Joint United National Programme on HIV/AIDS. Start free, stay free, AIDS free-a super-fast-track framework for ending AIDS among children, adolescents and young women by 2020[R]. Geneva: The Joint United National Programme on HIV/AIDS, 2016. [4] 高爽, 汤柳英, 祝新红, 等. 2013-2015年广东省127例预防HIV母婴传播综合干预效果分析[J]. 中国艾滋病性病, 2018, 24(2): 125-127. DOI: 10.13419/j.cnki.aids.2018.02.06.Gao S, Tang LY, Zhu XH, et al. Effect analysis of integrated intervention for prevention of mother to child transmission of HIV/AID in Guangdong during 2013 and 2015[J]. Chin J AIDS STD, 2018, 24(2): 125-127. DOI: 10.13419/j.cnki.aids.2018.02.06. [5] 汤柳英, 高爽, 钟银莉, 等. 婴儿艾滋病感染早期诊断信息管理系统的应用与探索[J]. 中国妇幼卫生, 2017, 8(3): 87-89. DOI: 10.19757/j.cnki.issn1674-7763.2017.03.025.Tang LY, Gao S, Zhong YL, et al. Application and exploration of the early diagnosis of HIV-infected infants information management system[J]. Chinese Journal of Women and Children Health, 2017, 8(3): 87-89. DOI: 10.19757/j.cnki.issn1674-7763.2017.03.025. [6] 龚韩湘, 吴泽墉, 伍宝玲, 等. 广东省医疗卫生资源空间聚集特征评价分析[J]. 中国卫生经济, 2017, 36(5): 52-55. DOI: 10.7664/CHE20170515.Gong HX, Wu ZY, Wu BL, et al. Analysis on spatial aggregation feature of health resources in Guangdong[J]. Chin Heal Econ, 2017, 36(5): 52-55. DOI: 10.7664/CHE20170515. [7] 中华人民共和国国家卫生和计划生育委员会. 国家卫生计生委办公厅关于全面开展预防艾滋病、梅毒和乙肝母婴传播工作的通知[J]. 国家卫生计生委公报, 2015, 4: 11-29.National Health and Family Planning Commission of People's Republic of China. Circular of the General Office of the National Health and Family Planning Commission on comprehensively carrying out the work of preventing mother-to-child transmission of AIDS, syphilis and hepatitis B[J]. Gazette of the National Health and Family Planning Commission of People's Republic of China, 2015, 4: 11-29. [8] 姜颖颖, 王前, 乔亚萍, 等. 我国4省区HIV感染孕产妇流行病学特征差异分析[J]. 中国健康教育, 2017, 33(7): 592-595. DOI: 10.16168/j.cnki.issn.1002-9982.2017.07.004.Jiang YY, Wang Q, Qiao YP, et al. The difference analysis of epidemiological characteristics among HIV infected pregnant women in 4 provinces, China[J]. Chin J Health Education, 2017, 33(7): 592-595. DOI: 10.16168/j.cnki.issn.1002-9982.2017.07.004. [9] Naiwatanakul T, Voramongkol N, Punsuwan N, et al. Uptake of early infant diagnosis in Thailand's national program for preventing mother-to-child HIV transmission and linkage to care, 2008-2011[J]. J Int AIDS Soc, 2016, 19(1): 20511. DOI: 10.7448/IAS.19.1.20511. [10] Achwoka D, Mandala J, Muriithi M, et al. Progress toward elimination of perinatal HIV transmission in Kenya: Analysis of early infant diagnosis data[J]. Int J STD AIDS, 2018, 29(7): 632-640. DOI: 10.1177/0956462417724015. [11] 叶俊. 我国基本医疗卫生制度改革研究[D]. 苏州: 苏州大学, 2016.Ye J. Research on the reform of basic medical and healthcare system of China[D]. Suzhou: Suzhou University, 2016. [12] Li B, Zhao QG, Zhang XZ, et al. Effectiveness of a prevention of mother-to-child transmission program in Guangdong province from 2007 to 2010[J]. BMC Public Health, 2013, 13: 591-597. DOI: 10.1186/1471-2458-13-591. [13] World Health Orgnization. Guidelines on HIV and infant feeding: principles and recommendations for infant feeding in the context of HIV and a summary of evidence[R]. Geneva: World Health Orgnization, 2010. [14] Nguyen TTV, Sabin K, Ho TQT, et al. Monitoring prevention impact of mother-to-child transmission of HIV in concentrated epidemics with program and survey data[J]. JMIR Public Health Surveill, 2017, 3(4): e76. DOI: 10.2196/publichealth.7701. [15] Ashinon E, Achwoka D, Mutugi J, et al. Vertical HIV transmission in perinatally-exposed infants in south-rift region of Kenya: a retrospective cross sectional study[J]. BMC Public Health, 2017, 17(1): 207-214. DOI: 10.1186/s12889-017-4124-z. [16] 王潇滟, 王爱玲, 王芳, 等. 高流行地区HIV感染产妇配偶HIV检测情况及影响因素分析[J]. 中国艾滋病性病, 2015, 21(6): 493-496. DOI: 10.13419/j.cnki.aids.2015.06.13.Wang XY, Wang AL, Wang F, et al. Partner's HIV testing and influence factors of HIV infected maternities in some high prevalence area of China[J]. Chin J AIDS STD, 2015, 21(6): 493-496. DOI: 10.13419/j.cnki.aids.2015.06.13. [17] World Health Organization. Appropriate technology for birth[J]. Lancet, 1985, 2(8452): 436-437. DOI: 10.1016/S0140-6736(85)92750-3. [18] Lumaca A, Galli L. de Martino M, et al. Paediatric HIV-1 infection: updated strategies of prevention mother-to-child transmission[J]. J Chemother, 2018, 30(4): 193-202. DOI: 10.1080/1120009X.2018.1451030. [19] 孔繁娟, 王璋华, 刘智昱, 等. 湖南省374例HIV感染孕产妇孕期及分娩情况[J]. 中国艾滋病性病, 2016, 22(9): 737-739. DOI: 10.13419/j.cnki.aids.2016.09.19.Kong FJ, Wang ZH, Liu ZY, et al. Pregnancy and delivery of 374 HIV infected women in Hunan Province[J]. Chin J AIDS STD, 2016, 22(9): 737-739. DOI:10.13419/j.cnki.aids. 2016.09.19. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 238
- HTML全文浏览量: 159
- PDF下载量: 23
- 被引次数: 0