

The prognostic effects of treatment on oral cancer patients with T1-4N0M0 stage
-
摘要:
目的 探讨治疗方式对T1-4N0M0期口腔癌患者预后的影响。 方法 收集2010年10月-2017年6月在福建医科大学附属第一医院口腔颌面外科经病理确诊的新发口腔癌患者, 所有的患者淋巴结病理诊断结果均呈阴性且未发生远处转移。采用单因素及多因素Cox比例风险模型进行预后影响因素的分析。 结果 本研究共纳入454名研究对象, 分析结果显示手术联合化疗(HR=1.792, 95% CI:1.025~3.134, P=0.041)的患者及手术联合放化疗(HR=2.111, 95% CI:1.275~3.495, P=0.004)的患者相比于单纯手术治疗患者预后更差。分层分析结果显示, 在淋巴结清扫总数为10~31个、BMI≥24.0 kg/m2的患者中:手术联合放疗相比于单纯手术治疗对患者预后更差; 在淋巴结清扫总数为32~87个、BMI < 18.5 kg/m2的患者中:手术联合化疗相比于单纯手术治疗对患者预后更差; 在淋巴结清扫总数10~31个、T分期T1-T2、BMI=18.5~23.9 kg/m2的患者中:手术联合放化疗相比于单纯手术治疗对患者预后更差。 结论 在T1-4N0M0口腔癌患者中, 手术联合放疗、手术联合化疗或手术联合放化疗相比于单纯手术治疗对患者的预后较差。 Abstract:Objective To investigate the effects of treatments for the prognosis of T1-4N0M0 stage oral cancer patients. Methods Patients with new oral cancer confirmed by pathology in the department of oral and maxillofacial surgery, the First Affiliated Hospital of Fujian Medical University from October 2010 to June 2017 were recruited in the study. The pathological diagnosis of lymph nodes was negative, and no distant metastasis occurred in all patients. The univariate and multivariate Cox proportional risk model was used to analyze the prognostic factors of oral cancer. Results A total of 454 subjects were included in this study. The results showed that patients receiving surgery combined with chemotherapy(HR=1.792, 95% CI: 1.025-3.134, P=0.041) and patients receiving surgery combined with chemoradiotherapy(HR=2.111, 95% CI: 1.275-3.495, P=0.004) had worse prognosis compared with those receiving surgery alone. Stratified analysis showed that among the patients with the total number of lymph node was 10-31 or BMI ≥ 24.0 kg/m2: patients receiving surgery combined with radiotherapy have a worse prognosis compared with those receiving surgery alone. Among the patients with the total number of lymph node was 32-87 or clinical staging Ⅰ-Ⅱ and BMI < 18.5 kg/m 2: patients receiving surgery combined with chemotherapy had a worse prognosis compared with those receiving surgery alone. Among the patients with the total number of lymph node was 10-31, clinical staging Ⅰ-Ⅱ or BMI < 18.5 kg/m 2: patients receiving surgery combined with chemoradiotherapy had a worse prognosis compared with those receiving surgery alone. Conclusion Among the T1-4N0M0 patients with oral cancer, receiving surgery combined with radiotherapy, the patients receiving surgery combined with chemotherapy or receiving surgery combined with chemoradiotherapy have a worse prognosis compared with those receiving surgery alone. -
Key words:
- Oral cancer /
- Therapy method /
- Progress free survival
-

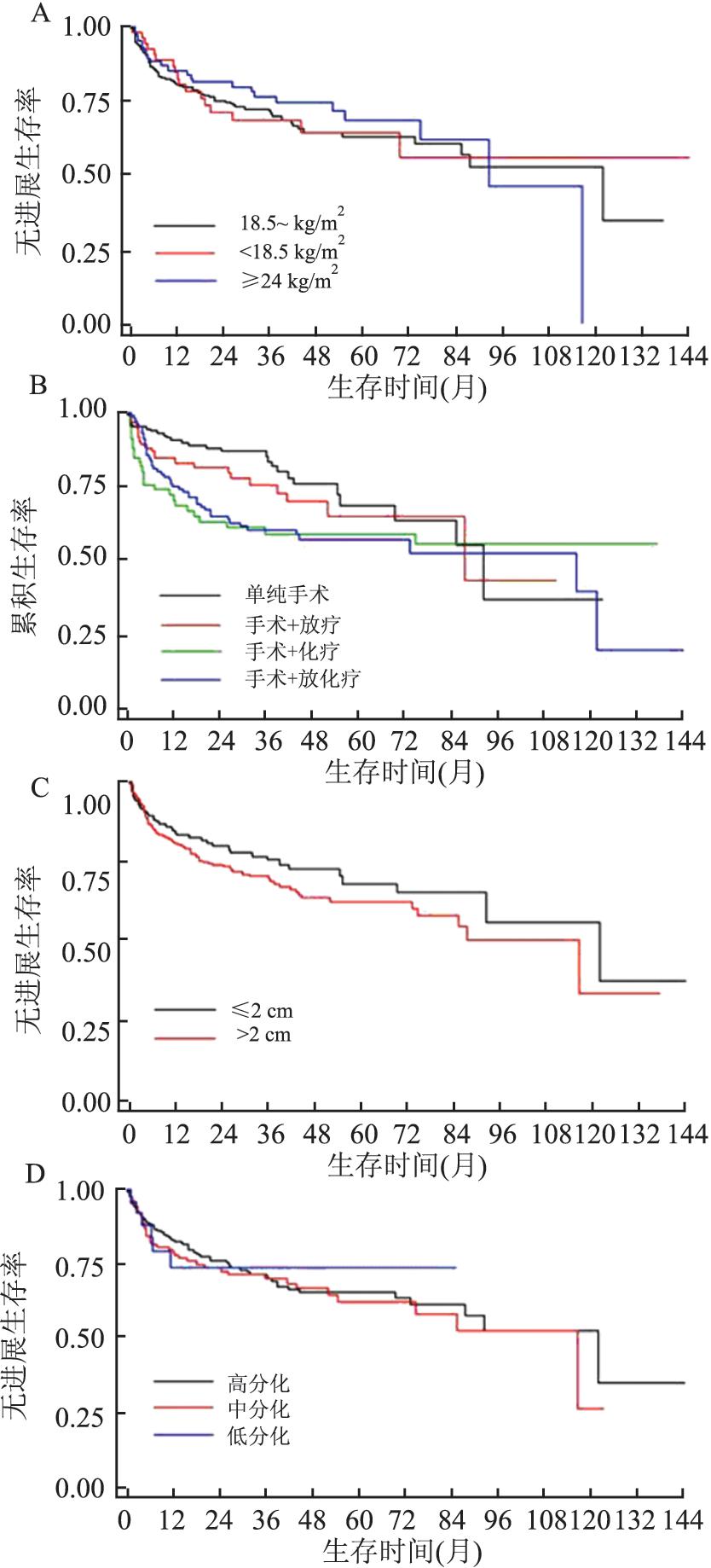
图 1 T1-4N0M0期口腔癌患者PFS的生存曲线图
Figure 1. Survival curve of PFS in patients with oral cancer at stage T1-4N0M0
表 1 T1-4N0M0期口腔癌患者PFS的单因素分析[n(%)]
Table 1. Univariate analysis of PFS in patients with T1-4N0M0 oral cancer[n(%)]
特征 观察例数 删失数 进展例数 HR(95% CI)值 P值 性别 男 283 208(63.22) 75(60.00) 1.000 0.528 女 171 121(36.78) 50(40.00) 1.108(0.773~1.589) 年龄(岁) < 55 168 130(39.51) 38(30.40) 1.000 0.055 ≥55 286 199(60.49) 87(69.60) 1.470(1.002~2.156) 职业 农民 154 98(29.79) 56(44.80) 1.000 0.009 工人 97 68(20.67) 29(23.20) 0.713(0.454~1.118) 其他 203 163(49.54) 40(32.00) 0.523(0.348~0.787) 居住地 城市 200 146(44.38) 54(43.20) 1.000 0.645 农村 251 181(55.01) 70(56.00) 1.200(0.841~1.714) 缺失 3 2(0.61) 1(0.80) 文化程度 文盲 29 25(7.60) 4(3.20) 1.000 0.118 小学和初中 323 223(67.78) 100(80.00) 2.130(0.783~5.793) 高中以上 75 62(18.84) 13(10.40) 1.187(0.387~3.643) 缺失 27 19(5.78) 8(6.40) BMI(kg/m2) 18.5~ 286 206(62.61) 80(64.00) 1.000 0.662 < 18.5 58 40(12.16) 18(14.40) 1.037(0.621~1.729) ≥24 110 83(25.23) 27(21.60) 0.819(0.529~1.267) 临床分期 Ⅰ~Ⅱ 234 167(50.76) 67(53.60) 1.000 0.725 Ⅲ~Ⅳ 200 149(45.29) 51(40.80) 0.880(0.611~1.267) 缺失 20 13(3.95) 7(5.60) 组织分化 高分化 253 180(54.71) 73(58.40) 1.000 0.541 中分化 129 89(27.05) 40(32.00) 1.107(0.753~1.629) 低分化 25 19(5.78) 6(4.80) 0.936(0.407~2.156) 缺失 47 41(12.46) 6(4.80) 治疗方式 单纯手术 167 138(41.95) 29(23.20) 1.000 0.011 手术+放疗 99 76(23.10) 23(18.40) 1.353(0.783~2.340) 手术+化疗 70 43(13.07) 27(21.60) 2.126(1.253~3.606) 手术+放化疗 118 72(21.88) 46(36.80) 2.004(1.257~3.194) 淋巴结清扫总数(个) 1~ 169 36(10.94) 13(10.40) 1.000 0.237 10~ 285 210(63.83) 85(68.00) 0.975(0.541~1.757) ≥32 83(25.23) 27(21.60) 0.881(0.451~1.718) 肿瘤最大径(cm) < 2 169 127(38.60) 42(33.60) 1.000 0.234 ≥2 285 202(61.40) 83(66.40) 1.223(0.843~1.773)  下载: 导出CSV
下载: 导出CSV
表 2 T1-4N0M0口腔癌患者PFS的多因素分析
Table 2. Multivariate analysis of PFS in patients with oral cancer T1-4N0M0
特征 HR(95% CI)值 P值 性别 男 1.000 女 1.142(0.772~1.690) 0.505 年龄(岁) < 55 1.000 ≥55 1.478(0.981~2.227) 0.062 居住地 城市 1.000 农村 0.908(0.536~1.539) 0.721 文化程度 文盲 1.000 初中 2.096(0.749~5.864) 0.159 高中以上 1.700(0.513~5.631) 0.385 职业 农民 1.000 工人 0.587(0.318~1.084) 0.089 其他 0.518(0.289~0.927) 0.027 临床分期 Ⅰ-Ⅱ 1.000 Ⅲ-Ⅳ 0.737(0.483~1.125) 0.158 BMI (kg/m2) 18.5~ 1.000 < 18.5 0.972(0.563~1.678) 0.920 ≥24 0.739(0.465~1.175) 0.201 肿瘤最大径(cm) < 2 1.000 ≥2 1.335(0.884~2.016) 0.169 淋巴结清扫总数(个) 1~ 1.000 10~ 0.888(0.464~1.702) 0.721 ≥32 0.800(0.383~1.670) 0.552 治疗方式 单纯手术 1.000 手术+放疗 1.606(0.901~2.864) 0.108 手术+化疗 1.792(1.025~3.134) 0.041 手术+放化疗 2.111(1.275~3.495) 0.004
下载: 导出CSV
表 3 不同治疗方式与T1-4N0M0期口腔癌患者PFS的分层分析结果
Table 3. 3 Stratified analysis of PFS in patients with T1-4N0M0 oral cancer by different treatment methods
变量 治疗方式 单纯手术 手术+放疗 手术+化疗 手术+放化疗手术+化疗 HR(95% CI)值 HR(95% CI)值 P值 HR(95% CI)值 P值 HR(95% CI)值 P值 淋巴结清扫总数a 1~ 1.000 0.171(0.017~1.756) 0.137 0.598(0.083, 4.321) 0.610 0.478(0.085, 2.677) 0.401 10~ 1.000 1.997(1.048~3.804) 0.035 1.509(0.769, 2.958) 0.232 2.028(1.134, 3.628) 0.017 ≥32 1.000 1.606(0.254~10.141) 0.614 7.621(1.506, 38.579) 0.014 4.445(0.879, 22.487) 0.071 BMI(kg/m2)b 18.5~ 1.000 1.288(0.606~2.736) 0.511 1.763(0.886, 3.508) 0.106 1.905(1.047, 3.465) 0.035 < 18.5 1.000 3.241(0.543~19.349) 0.197 6.238(1.290, 30.154) 0.023 5.499(0.955, 31.672) 0.056 ≥24 1.000 3.806(1.000~14.484) 0.050 2.739(0.673, 11.142) 0.159 2.254(0.641, 7.920) 0.205 T分期c T1~T2 1.000 1.621(0.772~3.405) 0.202 1.846(0.968, 3.519) 0.063 2.150(1.146, 4.031) 0.017 T3~T4 1.000 1.722(0.578~5.127) 0.395 2.260(0.678, 7.538) 0.308 2.458(0.908, 6.545) 0.047 注:a调整了肿瘤最大径、性别、居住地、年龄分组、临床分级、职业、文化程度、组织学分级、BMI; b调整了肿瘤最大径、性别、居住地、年龄分组、淋巴结总数、职业、文化程度、组织学分级、临床分级; c调整了肿瘤最大径、性别、居住地、年龄分组、淋巴结总数、职业、文化程度、组织学分级、BMI。
下载: 导出CSV
-
[1] Weng CJ, Hsieh YH, Chen MK, et al. Survivin SNP, carcinogen Interactions in Oral Cancer[J]. Journal of Dental Research, 2012, 91(4): 358-363. DOI: 10.1177/0022034512438402. [2] Mair M, Nair D, Nair S, et al. Comparison of tumor volume, thickness, and T classification as predictors of outcomes in surgically treated squamous cell carcinoma of the oral tongue[J]. Head & Neck, 2018, 40(8): 1667-1675. DOI: 10.1002/hed.25161. [3] Rajappa SK, Maheshwari U, Jaipuria J, et al. Number of positive nodes-Current relevance in determining prognosis of oral cavity cancer after the recent AJCC staging update[J]. Oral oncology, 2019, 90: 1-5. DOI: 10.1016/j.oraloncology.2019.01.001. [4] Chen F, Lin L, Liu F, et al. Three prognostic indexes as predictors of response to adjuvant chemoradiotherapy in patients with oral squamous cell carcinoma after radical surgery: A large‐scale prospective study[J]. Head & Neck, 2019, 41(2): 301-308. DOI: 10.1002/hed.25495. [5] Lee A, Givi B, Osborn VW, et al. Patterns of care and survival of adjuvant radiation for major salivary adenoid cystic carcinoma[J]. The Laryngoscope, 2017, 127(9): 2057-2062. DOI: 10.1002/lary.26516. [6] Liu F, Chen F, Huang J, et al. Prospective study on factors affecting the prognosis of oral cancer in a Chinese population[J]. Oncotarget, 2016, 8(3): 4352-4359. DOI: 10.18632/oncotarget.13842. [7] 李金忠, 李鑫, 郑家伟.早期口腔癌检查及诊断方法的研究进展[J].中国口腔颌面外科杂志, 2012, 10(6): 516-521. http://www.cnki.com.cn/Article/CJFDTotal-ZGKQ201206014.htmLi JZ, Li X, Zheng JW, et al. Advances in detection and diagnosis of early oral cancers[J]. China Journal of Oral and Maxillofacial Surgery, 2012, 10(6): 516-521. http://www.cnki.com.cn/Article/CJFDTotal-ZGKQ201206014.htm [8] Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab for squamous, cell carcinoma of the head and neck[J]. N Engl J Med, 2006, 354(6): 567-578. DOI: 10.1056/NEJMoa053422. [9] Wang L, Li H, Yang ZY, et al. Outcomes of primary squamous cell carcinoma of major salivary glands treated by surgery with or without postoperative radiotherapy[J]. Oral Maxillofac. Surg, 2015, 73: 1860-1864. DOI: 10.1016/j.joms.2015.03.016. [10] Gore SM, Crombie AK, Batstone MD, et al. Concurrent chemoradiotherapy compared with surgery and adjuvant radiotherapy for oral cavity squamous cell carcinoma[J]. Head & Neck, 2015, 37(4): 518-523. DOI: 10.1002/hed.23626. [11] 沈坤炜, 沈镇宙, 韩企夏. 1484例腋淋巴结阴性乳腺癌患者预后的多因素Cox模型分析[J].中华肿瘤杂志, 1997, 19(3): 221-224. http://www.cnki.com.cn/Article/CJFDTotal-ZHZL703.027.htmShen KW, Shen ZY, Han QX. Cox proportion hazard model multivariate analysis of prognosis of 1484 axillary node, negative breast cancer patients[J]. Chin J Oncol, 1997, 19(3): 221-224. http://www.cnki.com.cn/Article/CJFDTotal-ZHZL703.027.htm [12] Gibson MK, Li Y, Murphy B, et al. Randomized phase III evaluation of cisplatin plus fluorouracil versus cisplatin plus paclitaxel in advanced head and neck cancer(E1395): an intergroup trial of the eastern cooperative oncology group[J]. J Clin Oncol, 2005, 23(15): 3562-3567. DOI: 10.1200/JCO.2005.01.057. [13] Langer CJ, Harris J, Horwitz EM, et al. Phase II study of low, dose paclitaxel and cisplatin in combination with split, course concomitant twice, daily reirradiation in recurrent squamous cell carcinoma of the head and neck: results of radiation therapy oncology group protocol 9911[J]. J Clin Oncol, 2007, 25(30): 4800-4805. DOI: 10.1200/JCO.2006.07.9194. [14] Arduino PG, Carrozzo M, Chiecchio A, et al. Clinical and histopathologic independent prognostic factors in oral squamous cell carcinoma: a retrospective study of 334 cases[J]. J Oral Maxillofac Surg, 2008, 66(8): 1570-1579. DOI: 10.1016/j.joms.2007.12.024. [15] Saito N, Imai Y, Muto T, et al. Low body mass index as a risk factor of moderate to severe oral mucositis in oral cancer patients with radiotherapy[J]. Support Care Cancer, 2012, 20(12): 3373-3377. DOI: 10.1007/s00520-012-1620-7. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 260
- HTML全文浏览量: 148
- PDF下载量: 25
- 被引次数: 0