

Study on the relationship between early clinical symptoms and prognosis of Japanese encephalitis: based on Group LASSO Logistic regression model
-
摘要:
目的 探索Group LASSO (least absolute shrinkage and selection operator) Logistic回归分析模型在研究流行性乙型脑炎(简称乙脑)早期临床症状与预后之间的关系中的应用。 方法 收集整理2017-2018年甘肃省乙脑报告发病数据,建立乙脑预后影响因素的Group LASSO Logistic回归分析模型,通过交叉验证法选择惩罚参数,筛选出影响乙脑预后的早期临床症状。 结果 纳入的866名乙脑患者中,有预后结局的共764名,其中死亡者占22.5%、有后遗症者占12.6%、好转者占17.8%、痊愈者占47.1%。筛选出的变量有意识障碍、呼吸衰竭、呼吸节律改变、肌张力增强及乙脑疫苗接种史。 结论 通过构建Group LASSO Logistic回归分析模型可以筛选出对预后有影响的早期临床症状。 -
关键词:
- Group LASSO Logistic回归分析模型 /
- 流行性乙型脑炎 /
- 早期临床症状 /
- 预后
Abstract:Objective To explore the application of Group least absolute shrinkage and selection operator (LASSO) Logistic regression model in the study of the relationship between early clinical symptoms and prognosis of Japanese encephalitis (JE). Methods The data on JE in Gansu Province between 2017 to 2018 were collected from the infectious diseases system of China information system for diseases control and prevention. The Group LASSO Logistic regression model of the prognostic factors of JE was established. Punishment parameters were selected through the cross-validation method to screen out early symptoms that affect the prognosis of JE. Results Of the 866 included JE patients, 764 had prognostic outcomes, of which 22.5% were dead, 12.6% had sequelae, 17.8% were improved, and 47.1% were cured. The selected variables were consciousness disorder, respiratory failure, changes in respiratory rhythm, increased muscle tone, and history of JE vaccination. Conclusion Group LASSO Logistic regression model could be used to screen out early clinical symptoms that have an impact on the prognosis, which is of great significance for early detection of patients who may have a poor prognosis. -

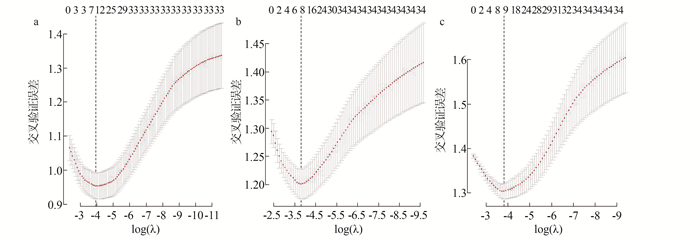
图 1 惩罚参数λ的对数与模型误差的关系
Figure 1. The relationship between the logarithm of penalty parameter and model error
表 1 甘肃省2017-2018年报告乙脑病例的人群分布特征
Table 1. Population distribution of cases reported in Gansu Province from 2017 to 2018
类别 2017年 2018年 合计 n
(例)构成比
(%)n
(例)构成比
(%)n
(例)构成比
(%)性别 男 178 49.2 237 47.0 415 47.9 女 184 50.8 267 53.0 451 52.1 年龄(岁) 0~ < 15 12 3.3 17 3.4 29 3.3 15~ < 65 273 75.4 322 63.9 595 68.7 ≥65 77 21.3 165 32.7 242 27.9 职业 农民 284 78.5 420 83.3 704 81.3 学生 29 8.0 24 4.8 53 6.1 家政、家务及待业人员 12 3.3 15 3.0 27 3.1 离退休人员 5 1.4 18 3.6 23 2.7 其他 32 8.8 27 5.4 59 6.8  下载: 导出CSV
下载: 导出CSV
表 2 成功随访组与失访组的基线资料比较[n(%)]
Table 2. Comparison of baseline data between follow-up group and lost group [n(%)]
类别 随访
(n=764)失访
(n=102)χ2值 P值 性别 0.034 0.853 男 367(88.4) 48(11.6) 女 397(88.0) 54(12.0) 年龄(岁) 9.351 0.009 0~ < 15 21(72.4) 8(27.6) 15~ < 65 522(87.7) 73(12.3) ≥65 221(91.3) 21(8.7) 职业 7.859 0.097 农民 630(89.5) 74(10.5) 学生 43(81.1) 10(18.9) 家政、家务及待业 24(88.9) 3(11.1) 离退休人员 20(87.0) 3(13.0) 其他 47(79.7) 12(20.3)
下载: 导出CSV
表 3 影响乙脑预后的早期临床症状的单因素分析
Table 3. Univariate analysis of early clinical symptoms affecting prognosis of Japanese encephalitis
变量 分类 病情转归 H值 P值 死亡
(n=172)有后遗症
(n=96)好转
(n=136)痊愈
(n=360)起病急 不详(X1A) 0 0 0 7 8.017 0.018 有(X1B) 160 87 124 317 无(X1C) 12 9 12 36 发热 不详(X2A) 1 1 0 3 2.672 0.263 有(X2B) 166 94 133 340 无(X2C) 5 1 3 17 发热温度 发热不详(X3A) 1 1 0 3 9.208 0.101 发热,温度不详(X3B) 1 0 0 4 >40 ℃(X3C) 18 14 11 37 39~≤40 ℃(X3D) 114 55 91 199 <39 ℃(X3E) 33 25 31 100 无发热(X3F) 5 1 3 17 头痛 不详(X4A) 15 6 6 15 5.167 0.076 有(X4B) 125 69 101 283 无(X4C) 32 21 29 62 头晕 不详(X5A) 18 4 10 17 9.643 0.008 有(X5B) 108 46 76 191 无(X5C) 46 46 50 152 腹痛 不详(X6A) 8 5 4 12 0.889 0.641 有(X6B) 17 8 15 32 无(X6C) 147 83 117 316 腹泻 不详(X7A) 6 3 4 7 3.272 0.195 有(X7B) 16 4 14 20 无(X7C) 150 89 118 333 恶心 不详(X8A) 5 1 1 7 0.163 0.922 有(X8B) 95 40 85 194 无(X8C) 72 55 50 159 呕吐 不详(X9A) 3 0 1 6 1.060 0.589 有(X9B) 87 37 64 158 无(X9C) 82 59 71 196 喷射性呕吐 不详(X10A) 13 5 12 16 3.144 0.370 有(X10B) 13 2 9 17 无(X10C) 64 30 44 131 无呕吐(X10D) 82 59 71 196 精神萎靡 不详(X11A) 4 1 1 6 7.371 0.025 有(X11B) 149 78 106 276 无(X11C) 19 17 29 78 易激惹 不详(X12A) 6 4 5 15 1.006 0.605 有(X12B) 54 27 43 98 无(X12C) 112 65 88 247 嗜睡 不详(X13A) 3 3 2 7 19.651 <0.001 有(X13B) 130 54 85 193 无(X13C) 39 39 49 160 烦躁 不详(X14A) 5 2 1 9 5.288 0.071 有(X14B) 95 49 77 164 无(X14C) 72 45 58 187 惊厥 不详(X15A) 7 2 3 11 22.459 <0.001 有(X15B) 57 20 34 53 无(X15C) 108 74 99 296 意识障碍 不详(X16A) 2 0 0 5 62.831 <0.001 有(X16B) 146 64 86 176 无(X16C) 24 32 50 179 抽搐 不详(X17A) 7 3 5 13 26.631 <0.001 反复或持续性强烈抽搐(X17B) 10 1 2 10 反复抽搐(X17C) 18 9 6 13 局部肌肉小抽搐(X17D) 43 13 26 46 无(X17E) 94 70 97 278 呼吸衰竭 不详(X18A) 2 1 1 3 56.951 <0.001 有(X18B) 55 11 9 21 无(X18C) 115 84 126 336 循环衰竭 不详(X19A) 4 3 3 3 10.036 0.007 有(X19B) 12 0 1 6 无(X19C) 156 93 132 351 血压改变 不详(X20A) 7 5 7 14 27.303 <0.001 升高(X20B) 54 34 29 56 降低(X20C) 11 3 6 13 正常(X20D) 100 54 94 277 呼吸节律改变 不详(X21A) 2 2 6 4 43.502 <0.001 有(X21B) 67 16 20 43 无(X21C) 103 78 110 313 瞳孔大小改变 不详(X22A) 3 1 3 5 11.262 0.004 有(X22B) 27 5 7 20 无(X22C) 142 90 126 335 脑膜刺激征 不详(X23A) 1 5 5 8 4.770 0.092 有(X23B) 96 41 76 160 无(X23C) 75 50 55 192 前囟膨隆 不详(X24A) 6 3 6 10 0.446 0.800 有(X24B) 2 1 0 5 无(X24B) 164 92 130 345 腹壁反射 不详(X25A) 9 8 9 17 0.517 0.772 有(X25B) 95 60 82 210 无(X25C) 68 28 45 133 提睾反射 不详(X26A) 18 10 10 31 1.181 0.757 女(X26B) 86 43 77 191 有(X26C) 39 31 37 89 无(X26D) 29 12 12 49 肌张力增强 不详(X27A) 7 4 8 6 36.506 <0.001 有(X27B) 80 30 45 80 无(X27C) 85 62 83 274 巴宾斯基征 不详(X28A) 5 5 7 9 13.496 0.001 有(X28B) 59 19 30 67 无(X28C) 108 72 99 284 支气管肺炎 不详(X29A) 6 4 4 7 10.074 0.006 有(X29B) 34 14 19 38 无(X29C) 132 78 113 315 肺不张 不详(X30A) 6 2 5 9 4.336 0.114 有(X30B) 3 2 0 1 无(X30B) 163 92 131 350 败血症 不详(X31A) 7 3 4 8 3.467 0.177 有(X31B) 1 0 0 0 无(X31C) 164 93 132 352 胃肠道出血 不详(X32A) 7 5 4 8 2.134 0.344 有(X32B) 0 1 0 1 无(X32C) 165 90 132 351 尿路感染 不详(X33A) 7 2 4 9 0.637 0.727 有(X33B) 3 2 0 6 无(X33C) 162 92 132 345 乙脑疫苗接种史 不详(X34A) 49 37 48 113 9.384 0.009 有(X34B) 0 0 3 13 无(X34C) 123 59 85 234
下载: 导出CSV
-
[1] 李兰娟, 任红. 传染病学[M]. 第8版. 北京: 人民卫生出版社, 2013: 86-92.Li LJ, Ren H. Infectious diseases[M]. 8rd ed. Beijing: People's Medical Publishing House, 2013: 86-92. [2] 汪倩. 儿童重症流行性乙型脑炎临床特点及预后分析[D]. 重庆: 重庆医科大学, 2019.Wang Q. Clinical features and prognostic analysis of severe Japanese B encephalitis in children[D]. Chongqing: Chongqing Medical University, 2019. [3] 张蕾洁, 金娜, 王琪, 等. Bayes综合判别对流行性乙型脑炎临床分型的鉴别[J]. 中华流行病学杂志, 2019, 40(9): 1164-1167. DOI: 10.3760/cma.j.issn.0254-6450.2019.09.028.Zhang LJ, Jin N, Wang Q, et al. Study on clinical classification of Japanese encephalitis by Bayes discriminant analysis[J]. Chin J Epidemiol, 2019, 40(9): 1164-1167. DOI: 10.3760/cma.j.issn.0254-6450.2019.09.028. [4] 方匡南, 章贵军, 张惠颖. 基于Lasso-logistic模型的个人信用风险预警方法[J]. 数量经济技术经济研究, 2014, 31(2): 125-136. DOI: 10.13653/j.cnki.jqte.2014.02.009.Fang KN, Zhang GJ, Zhang HY. Individual credit risk prediction method: application of a lasso-logistic model[J]. J Quant Tech Econ, 2014, 31(2): 125-136. DOI: 10.13653/j.cnki.jqte.2014.02.009. [5] Tibshirani R. Regression shrinkage and selection via the lasso[J]. J Royal Stat Soc: Ser B Methodol, 1996, 58(1): 267-288. DOI: 10.1111/j.2517-6161.1996.tb02080.x. [6] Yuan M, Lin Y. Model selection and estimation in regression with grouped variables[J]. J Royal Stat Soc: Ser B Stat Methodol, 2006, 68(1): 49-67. DOI: 10.1111/j.1467-9868.2005.00532.x.. [7] 金娜, 张晓曙, 张秉玲, 等. 甘肃省2004—2017年流行性乙型脑炎发病及流行特征[J]. 中国公共卫生, 2020, 36(2): 210-214. DOI: 10.11847/zgggws1121131.Jin N, Zhang XS, Zhang BL, et al. Incidence trend and prevalence status of Japanese encephalitis in Gansu Province, 2004-2017[J]. Chin J Public Heal, 2020, 36(2): 210-214. DOI: 10.11847/zgggws1121131. [8] 中华人民共和国卫生部. WS 214-2008流行性乙型脑炎诊断标准[S]. 北京: 人民卫生出版社, 2009.Ministry of Health of the People's Republic of China. WS 214-2008 Diagnostic criteria for Japanese encephalitis[S]. Beijing: People's Medical Publishing House, 2009. [9] 陈茹, 王晶, 唐少文, 等. 抗结核治疗队列人群药物性肝损害的易感基因多态性研究[J]. 中华流行病学杂志, 2016, 37(7): 925-929. DOI: 10.3760/cma.j.issn.0254-6450.2016.07.004.Chen R, Wang J, Tang SW, et al. Study on polymorphisms of genes with susceptibility to drug induced liver injury in a cohort receiving anti-tuberculosis treatment[J]. Chin J Epidemiol, 2016, 37(7): 925-929. DOI: 10.3760/cma.j.issn.0254-6450.2016.07.004. [10] 李泱. 兰州市高血压患病情况的调查分析及模型选择[D]. 兰州: 兰州大学, 2016.Li Y. Investigation analysis and model selection of the prevalence of hypertension in Lanzhou city[D]. Lanzhou: Lanzhou University, 2016. [11] Meier L, van de Geer S, Bühlmann P. The group lasso for logistic regression[J]. J Royal Stat Soc: Ser B Stat Methodol, 2008, 70(1): 53-71. DOI: 10.1111/j.1467-9868.2007.00627.x. [12] 张啸, 赵薇, 胡焕青, 等. 基于group lasso logistic回归的6月龄婴儿贫血预测模型的构建[J]. 中国慢性病预防与控制, 2020, 28(3): 199-205. DOI: 10.16386/j.cjpccd.issn.1004-6194.2020.03.009.Zhang X, Zhao W, Hu HQ, et al. Construction of predictive model for Anemia in 6-month-old infants on the basis of group lasso logistic regression[J]. Chin J Prev Control Chronic Dis, 2020, 28(3): 199-205. DOI: 10.16386/j.cjpccd.issn.1004-6194.2020.03.009. [13] 成娟, 梁轩, 郑森爽, 等. 基于Lasso Logistic回归模型的乳腺癌高风险人群筛查利用相关因素研究[J]. 中华疾病控制杂志, 2018, 22(6): 551-554, 559. DOI: 10.16462/j.cnki.zhjbkz.2018.06.003.Cheng J, Liang X, Zheng SS, et al. Predictors of breast cancer screening utilization among female at high risk of developing breast cancer: application of a Lasso Logistic model[J]. Chin J Dis Control Prev, 2018, 22(6): 551-554, 559. DOI: 10.16462/j.cnki.zhjbkz.2018.06.003. [14] 刘芹. 儿童流行性乙型脑炎预后危险因素的Meta分析[D]. 重庆: 重庆医科大学, 2018.Liu Q. Meta-analysis of the risk factors for prognosis of Japanese encephalitis in children[D]. Chongqing: Chongqing Medical University, 2018. [15] 王阿美. 104例流行性乙型脑炎患者临床特点及预后影响因素分析[D]. 银川: 宁夏医科大学, 2020.Wang AM. Clinical characteristics and prognostic risk factors of 104 Japanese encephalitis cases[D]. Yinchuan: Ningxia Medical University, 2018. [16] Kakoti G, Dutta P, Ram Das B, et al. Clinical profile and outcome of Japanese encephalitis in children admitted with acute encephalitis syndrome[J]. Biomed Res Int, 2013, 2013: 152656. DOI: 10.1155/2013/152656. [17] Sunwoo JS, Lee ST, Jung KH, et al. Clinical characteristics of severe Japanese encephalitis: a case series from south Korea[J]. Am J Trop Med Hyg, 2017, 97(2): 369-375. DOI: 10.4269/ajtmh.17-0054. [18] 张燕菊. 成人流行性乙型脑炎预后相关因素的分析[D]. 兰州: 兰州大学, 2019.Zhang JY. Analysis of prognostic factors in adult Japanese encephalitis[D]. Lanzhou: Lanzhou University, 2019. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 613
- HTML全文浏览量: 231
- PDF下载量: 144
- 被引次数: 0