

Investigation on infectious disease-specific health literacy of Chinese expatriates in engineering construction enterprises
-
摘要:
目的 了解中国工程建设企业海外员工的传染病健康素养水平及其影响因素,为中资企业海外员工传染病防治工作提供依据。 方法 采取整群抽样,选取某大型石油公司所属工程建设企业2019年9月-12月参加出国培训的员工,采用自行设计的传染病健康素养问卷进行调查。 结果 员工传染病健康素养水平为51.5%。单因素分析显示,女性员工传染病健康素养高于男性(χ2 =4.559, P=0.045),年龄<50岁者高于年龄≥50岁者(χ2 =6.027, P=0.015),管理人员高于操作人员(χ2 =53.025, P<0.001)。多因素分析显示,文化程度和职业类型是影响传染病健康素养的主要因素。相较小学文化程度,初中(OR=3.847, 95% CI: 0.476~31.086, P=0.206)、高中/中专/职高(OR=7.439, 95% CI: 0.932~59.377, P=0.058)、大专/本科(OR=15.887, 95% CI: 1.992~126.673, P=0.009)、硕士及以上(OR=14.581, 95% CI: 1.681~126.479, P=0.015)者传染病健康素养较高;管理人员素养高于操作人员(OR=1.588, 95% CI: 1.105~2.281, P=0.012)。 结论 工程建设企业海外员工的传染病健康素养水平较低,主要影响因素为文化程度、职业类型和年龄。建议企业在员工出国前开展传染病防治的健康教育,重点教育对象应为高中及以下学历者、操作人员和≥50岁员工。 Abstract:Objective To investigate the infectious disease-specific health literacy (IDSHL) level of Chinese expatriates in engineering construction enterprises and its influencing factors, providing evidence-based recommendation for infection prevention and control practices. Methods A cluster sampling design was adopted to select employees of China National Petroleum Pipeline Engineering Corporation who participated in overseas training from September to December 2019. A self-designed questionnaire was conducted to explore the IDSHL level and influencing factors among employees. Results Overall, the employee's IDSHL rate was 51.5%. Univariate analysis showed that the IDSHL rate of female employees was higher than that of male employees (χ2 =4.559, P=0.045), IDSHL rate of those aged < 50 was higher than those aged ≥50 (χ2 =6.027, P=0.015), and IDSHL rate of managers was higher than operators (χ2 =53.025, P < 0.001). Multivariate logistic regression analysis showed that education level and occupation type were the main factors influencing IDSHL. Compared with employees with primary school education, IDSHL rates were higher in those with junior high school (OR=3.847, 95% CI: 0.476-31.086, P=0.206), high school/technical secondary school/vocational high school (OR=7.439, 95% CI: 0.932-59.377, P=0.058), junior college/ university (OR=15.887, 95% CI: 1.992-126.673, P=0.009) education and those have master's degree or above (OR=14.581, 95% CI: 1.681-126.479, P=0.015). IDSHL rates of managers were higher than operators (OR=1.588, 95% CI: 1.105-2.281, P=0.012). Conclusion The IDSHL level of Chinese expatriates in engineering construction enterprises is relatively low, and the main influencing factors are education level, occupation type and age. Our study recommends that enterprises should carry out health education training on infectious diseases prevention and control before their employees go abroad. The training should pay more attention on those with high school education or less, operators and employees over 50 years old. -
Key words:
- Expatriates /
- Infectious disease /
- Health literacy
-
健康素养是个人获取或理解基本健康信息和服务,并运用这些信息和服务做出正确决策,以维护和促进自身健康的能力[1]。传染病健康素养是健康素养的一部分。健康素养和健康状况密切相关,低健康素养对生活方式、卫生服务利用和对干预的依从性带来负面影响,导致疾病的发病和患病率高、疾病预后差。2012年全国健康素养监测结果显示,中国居民健康素养较低,在6类健康问题中,传染病防治素养处于较低水平[2]。
中国“一带一路”倡议提出后,中资企业加快了“走出去”的步伐,截至2017年末,已有2.56万家中国企业在境外设立分支机构,境外企业员工总数达到339.3万人[3]。工程建设企业的海外派遣地主要分布在非洲、东南亚、拉丁美洲等地区,驻地可能存在多种新发传染病和被忽视热带病流行[4-6],这些疾病与中国流行的主要传染病种类并不重合[7]。中国员工从国内低风险地区转移至海外高风险地区工作,对上述传染病缺乏防护意识,对疾病易感性更高且容易发展为重症[8]。工程建设如建筑、管道铺设等多为室外作业,驻地附近居民区存在较多传染源;员工长时间暴露于蚊虫叮咬的环境,可能接触不洁饮用水和食物,构成多种传染病的传播途径;由于当地医疗条件差,一旦发病在海外医治困难,如防控不力可能造成大范围流行。这些因素均对员工的生命健康带来不同于国内工作环境的威胁。
在有传染病传播风险的环境中,传染病健康素养是影响疾病发生发展和预防、诊疗、转运等医疗卫生服务利用的关键因素[9],但目前国内外均缺乏对海外工程建设企业员工这一群体的传染病相关健康素养的介绍。中国既往的健康素养监测主要针对国内常住人口,只关注国内流行的传染病,不适用于评价在海外工作的群体,无法指导其健康宣教工作。因此,为更好地了解工程建设企业海外员工的传染病健康素养水平及其影响因素,本研究以工程施工建设为主要业务的某大型石油公司所属企业员工为主要研究对象,结合文献研究和企业既往感染情况,设计了针对海外工程建设企业员工的传染病健康素养问卷,并对该企业计划外派的员工开展调查。
1. 对象与方法
1.1 研究对象
某大型石油公司所属工程建设企业参加出国培训的员工,本研究通过了北京大学生物医学伦理委员会审查,编号:IRB00001052-19113。
1.2 方法
1.2.1 抽样方法
采取整群抽样,选取参加2019年9月-12月培训的所有员工。
1.2.2 调查方法
使用自行设计的《海外员工传染病健康素养问卷》,调查员工的一般社会人口学特征和传染病防治健康素养。问卷的传染病健康素养调查部分共计40个条目,分别从传染病防治知识、行为和技能3个维度开展调查,主要涉及传染病综合防治和疟疾、登革热、感染性腹泻防治4个部分。问卷的题型构成为28个单选题、12个多选题,其中针对传染病防治行为的题目为情景题,考察传染病防治技能的问题设置为读图、短文阅读、药品说明书阅读和计算等形式。调查使用电子问卷,每一期培训班开始上课前由组织者通过班级微信群发放问卷链接,要求被调查者立即填写并在规定时间内提交问卷。问卷设置为无缺失项方可提交。
1.2.3 判定标准
单选题和多选题回答选项与正确答案完全一致判定为回答正确,多选题错选、多选、漏选均判定为回答错误。问卷中被调查对象回答正确的题目数占总题目数的比例为正确回答率。正确回答率≥60%者视为具备健康素养,具备健康素养的人在调查对象中所占的比例为该人群的健康素养水平。
1.3 统计学方法
使用SPSS 18.0软件进行统计分析,分别对性别、年龄、文化程度、职业类型等进行单因素分析(χ2检验)。采用多因素Logistic回归分析模型分析影响因素,模型同时纳入性别、年龄、文化程度、职业类型四个因素,分别汇总各因素的OR值及95% CI值。检验水准α=0.05。
2. 结果
2.1 基本情况
向参加培训的978名员工发放调查问卷链接,回收问卷938份,应答率为95.9%。经过数据清洗得到有效问卷917份,有效率为97.8%。问卷填写时间的中位数为12.4 min。被调查者男性占95.9%,女性占4.1%,年龄均≤55岁,其中79.2%在30~<50岁之间。被调查者的文化程度为大专/本科占54.0%,高中/中专/职高占24.9%、初中占17.6%,小学或硕士及以上学历者较少。管理人员占32.6%,操作人员占67.4%。
2.2 问卷正确回答率情况
问卷中传染病健康素养问题共40个,接受调查的员工对这些问题的正确回答率呈负偏峰分布,中值为60.0%。正确回答率集中在40.0%~80.0%区间,这部分员工占总体的85.2%,能正确回答≥80.0%者仅占5.6%。见图 1。
 图 1 传染病健康素养问卷正确回答率情况Figure 1. Correct rate of infectious disease-specific health literacy questionnaire
图 1 传染病健康素养问卷正确回答率情况Figure 1. Correct rate of infectious disease-specific health literacy questionnaire2.3 传染病健康素养水平
接受调查的员工中有51.5%能正确回答≥60%问题,即具备传染病健康素养。单因素分析结果显示,女性员工的传染病健康素养水平高于男性,差异有统计学意义(χ2 =4.554, P=0.045);文化程度越高,传染病健康素养水平越高(χ2 =35.242, P<0.001),管理人员的健康素养水平高于操作人员(χ2 =53.025, P<0.001)。传染病健康素养水平在4个年龄组间的分布差异无统计学意义(χ2 =7.485, P=0.058)。年龄组间两两比较显示,年龄<50岁组的传染病健康素养水平高于年龄≥50岁组。见表 1。
表 1 调查对象的社会人口学特征和传染病健康素养水平分布情况Table 1. Demographic and sociological characteristics of respondents and their infectious disease-specific health literacy level变量 人数(例) 构成比(%) 健康素养水平(%) χ2值 P值 性别 4.559 0.045 男性 879 95.9 50.7 女性 38 4.1 68.4 年龄(岁) 7.485 0.058 18~<30 150 16.4 52.0 30~<40 414 45.1 54.3 40~<55 313 34.1 49.8 50~≤55 40 4.4 32.5 文化程度 35.242 <0.001 小学 11 1.2 9.1 初中 161 17.6 27.3 高中/中专/职高 228 24.9 39.0 大专/本科 462 50.4 50.4 硕士及以上 55 6.0 52.7 职业类型 53.025 <0.001 管理人员 299 32.6 68.9 操作人员 618 67.4 43.0 2.4 传染病健康素养的影响因素
以是否具备传染病健康素养作为因变量,将性别、年龄、文化程度、职业类型作为自变量同时纳入模型,进行Logistic回归分析模型分析。结果显示在调整其他因素后,文化程度和职业类型是传染病健康素养的主要影响因素。以小学文化程度为对照,高于小学文化程度者具备传染病健康素养的概率升高,管理人员具备传染病健康素养的可能性是操作人员的1.588倍。见表 2。
表 2 传染病健康素养影响因素的Logistic回归分析模型分析结果Table 2. Multivariate logistic analysis of the factors influencing the infectious disease-specific health literacy变量 β值 Wald χ2值 OR(95% CI)值 P值 性别 女性 1.000 男性 -0.380 0.984 0.684(0.323~1.449) 0.321 年龄(岁) 18~<30 1.000 30~<40 0.214 1.125 1.239(0.834~1.842) 0.289 40~<50 0.209 0.965 1.233(0.812~1.871) 0.326 50~≤55 -0.474 1.412 0.622(0.284~1.361) 0.235 文化程度 小学 1.000 初中 1.347 1.597 3.847(0.476~31.086) 0.206 高中/中专/职高 2.007 3.585 7.439(0.932~59.377) 0.058 大专/本科 2.765 6.816 15.887(1.992~126.673) 0.009 硕士及以上 2.680 5.911 14.581(1.681~126.479) 0.015 职业类型 操作人员 1.000 管理人员 0.462 6.242 1.588(1.105~2.281) 0.012 3. 讨论
中国工程建设企业每年派往海外的人数庞大,因传染病死亡的事件时有发生。对死亡个案进行回顾性分析发现,员工对疾病缺乏认知,防范意识淡薄,不及时寻求医疗帮助,延误治疗时机,导致疾病迅速进展至重症,是造成死亡的重要原因。大多数传染病是可预防、可治疗的,提前采取干预措施能减少可避免的死亡和健康损失。本研究的样本来自某大型国有公司所属工程建设企业员工,该企业海外业务主要分布在非洲、东南亚、中东等地区,常年外派员工超过3 000人,此次参加出国培训的员工多数计划赴非洲地区,员工受到海外传染病的威胁较为凸出。对他们的传染病健康素养现状和影响因素进行摸底调查,可为后续开展针对性干预提供依据,并为更广泛的企业海外员工和出国劳务人员的传染病健康素养研究提供参考。
本次调查发现,该企业计划派往海外的员工中约有50%不具备传染病健康素养。受调查者的正确回答率集中在40%~80%之间,≥80%者仅占总体的5.6%,员工整体传染病防治健康素养水平较低。影响员工传染病健康素养的主要因素是职业类型和文化程度,文化程度低于高中/中专/职高、从事操作工作的群体传染病健康素养更为薄弱。职业类型和文化程度之间具有较高相关性和一定因果关系,由于文化程度高者更多从事管理工作,二者并非相互独立的影响因素,其中文化程度起着最重要和基础的作用,它对健康素养的决定性影响已在许多研究中得到证实[10]。因此,在海外员工传染病健康素养评价中,文化程度低可作为识别高危人群的最关键因素。
中资工程建设企业向海外派遣的员工以男性青年为主[11],本调查发现<50岁各年龄组员工的传染病健康素养水平差异不大,仅≥50岁组低于其他各组。可认为年龄对≥50岁群体传染病健康素养的影响更为明显,单因素分析和多因素回归分析结果均支持这一推断。健康素养的一个重要组成部分是健康信息素养,在多渠道特别是通过网络获取健康信息方面老年群体处于劣势,这种劣势将进一步影响健康素养[12-13]。在韩国全国开展的调查也显示,低健康素养的状况普遍出现在≥50岁的人群中[14]。因此,对于海外员工群体,年龄≥50岁也是值得注意的与低传染病健康素养相关的关键因素。
本研究结果提示工程建设企业海外员工的传染病健康素养有待提高,特别是低学历和高年龄工作者,应当通过有效的方式改善其传染病健康素养。既往关于呼吸道传染病健康素养和健康行为的决定因素研究[9]显示,教育对先验知识有正向的、直接的影响,而先验知识又影响着健康素养。另外国内多项针对出国劳务人员或旅行者的疟疾相关知识、态度和行为调查[11, 15]也显示,是否了解过疟疾知识与疟疾知识合格率相关,提示提前进行健康教育能提高出国人员对疾病的知晓率,并进一步影响防治态度和行为从而降低发病率[16]。综上所述,建议工程建设企业在员工出国前通过健康教育的方式提高其传染病健康素养,重点关注人群应为高中及以下学历者、操作人员和≥50岁员工,以保障他们在海外工作期间的健康和生命安全。另一方面,做好海外传染病防控工作,提高员工自我症状监测能力和对异常情况主动申报意识,也能降低员工回国时将疾病输入国内的可能性,对中国防控输入性传染病具有重要意义。
-
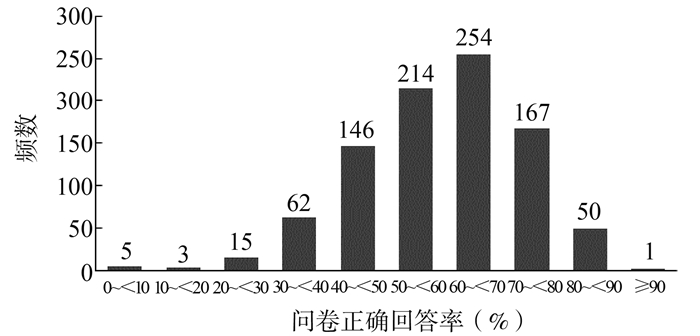
图 1 传染病健康素养问卷正确回答率情况
Figure 1. Correct rate of infectious disease-specific health literacy questionnaire
表 1 调查对象的社会人口学特征和传染病健康素养水平分布情况
Table 1. Demographic and sociological characteristics of respondents and their infectious disease-specific health literacy level
变量 人数(例) 构成比(%) 健康素养水平(%) χ2值 P值 性别 4.559 0.045 男性 879 95.9 50.7 女性 38 4.1 68.4 年龄(岁) 7.485 0.058 18~<30 150 16.4 52.0 30~<40 414 45.1 54.3 40~<55 313 34.1 49.8 50~≤55 40 4.4 32.5 文化程度 35.242 <0.001 小学 11 1.2 9.1 初中 161 17.6 27.3 高中/中专/职高 228 24.9 39.0 大专/本科 462 50.4 50.4 硕士及以上 55 6.0 52.7 职业类型 53.025 <0.001 管理人员 299 32.6 68.9 操作人员 618 67.4 43.0  下载: 导出CSV
下载: 导出CSV
表 2 传染病健康素养影响因素的Logistic回归分析模型分析结果
Table 2. Multivariate logistic analysis of the factors influencing the infectious disease-specific health literacy
变量 β值 Wald χ2值 OR(95% CI)值 P值 性别 女性 1.000 男性 -0.380 0.984 0.684(0.323~1.449) 0.321 年龄(岁) 18~<30 1.000 30~<40 0.214 1.125 1.239(0.834~1.842) 0.289 40~<50 0.209 0.965 1.233(0.812~1.871) 0.326 50~≤55 -0.474 1.412 0.622(0.284~1.361) 0.235 文化程度 小学 1.000 初中 1.347 1.597 3.847(0.476~31.086) 0.206 高中/中专/职高 2.007 3.585 7.439(0.932~59.377) 0.058 大专/本科 2.765 6.816 15.887(1.992~126.673) 0.009 硕士及以上 2.680 5.911 14.581(1.681~126.479) 0.015 职业类型 操作人员 1.000 管理人员 0.462 6.242 1.588(1.105~2.281) 0.012
下载: 导出CSV
-
[1] 健康中国行动推进委员会. 健康中国行动(2019-2030年)[EB/OL]. (2019-07-15)[2020-08-15]. http://www.gov.cn/xinwen/2019-07/15/content_5409694.htm.Promotion Committee of Healthy China Initiative. Healthy China initiative (2019-2030)[EB/OL]. (2019-07-15)[2020-08-15]. http://www.gov.cn/xinwen/2019-07/15/content_5409694.htm. [2] 李英华, 毛群安, 石琦, 等. 2012年中国居民健康素养监测结果[J]. 中国健康教育, 2015, 31(2): 99-103. DOI: 10.16168/j.cnki.issn.1002-9982.2015.02.001.Li YH, Mao QA, Shi Q, et al. The level of health literacy of Chinese residents in 2012: surveillance results[J]. Chin J Heal Educ, 2015, 31(2): 99-103. DOI: 10.16168/j.cnki.issn.1002-9982.2015.02.001. [3] 中华人民共和国商务部. 中国对外投资发展报告[R]. 2018. http://fec.mofcom.gov.cn/arricle/tzhzcj/tzhz/20190102831043.Ministry of Commerce People's Republic of China. Report on development of China's outward investment[R]. 2018. http://fec.mofcom.gov.cn/arricle/tzhzcj/tzhz/20190102831043. [4] 中国对外承包工程商会. 中国对外承包工程发展报告(2017-2018)[R]. 2019. https://www.chinca.org/CICA/info/19030614463611.China international contractors association. Annual Report on China International Project Contracting (2017-2018)[R]. 2019. https://www.chinca.org/CICA/info/19030614463611. [5] McArthur DB. Emerging infectious diseases[J]. Nurs Clin North Am, 2019, 54(2): 297-311. DOI: 10.1016/j.cnur.2019.02.006. [6] MacKey TK, Liang BA. Threats from emerging and re-emerging neglected tropical diseases (NTDs)[J]. Infect Ecol Epidemiol, 2012;2. DOI: 10.3402/iee.v2i0.18667. [7] 徐兰英, 余志祥. 2010-2016年中国大陆法定传染病流行特征分析[J]. 河南预防医学杂志, 2018, 29(4): 244-247, 291. DOI: 10.13515/j.cnki.hnjpm.1006-8414.2018.04.002.Xu LY, Yu ZX. Epidemiological features analysis of notifiable infectious diseases in mainland China, 2010-2016[J]. Henan J Prev Med, 2018, 29(4): 244-247, 291. DOI: 10.13515/j.cnki.hnjpm.1006-8414.2018.04.002. [8] Freedman DO, Chen LH, Kozarsky PE. Medical considerations before international travel[J]. N Engl J Med, 2016, 375(3): 247-260. DOI: 10.1056/nejmra1508815. [9] Sun XY, Shi YH, Zeng QQ, et al. Determinants of health literacy and health behavior regarding infectious respiratory diseases: a pathway model[J]. BMC Public Health, 2013, 13: 261. DOI: 10.1186/1471-2458-13-261. [10] 李莉, 李英华, 聂雪琼, 等. 2012年中国居民健康素养影响因素分析[J]. 中国健康教育, 2015, 31(2): 104-107. DOI: 10.16168/j.cnki.issn.1002-9982.2015.02.002.Li L, Li YH, Nie XQ, et al. Influence factors of health literacy monitoring of Chinese residents on 2012[J]. Chin J Heal Educ, 2015, 31(2): 104-107. DOI: 10.16168/j.cnki.issn.1002-9982.2015.02.002. [11] 李伟, 郭艳军, 韩乐强, 等. 驻尼日尔劳务人员疟疾相关健康素养及影响因素分析[J]. 现代预防医学, 2016, 43(19): 3551-3555. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYF201619028.htmLi W, Guo YJ, Han LQ, et al. Chinese laborers' malaria health literacy and related factors, Niger[J]. Mod Prev Med, 2016, 43(19): 3551-3555. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYF201619028.htm [12] Cutilli CC, Simko LC, Colbert AM, et al. Health literacy, health disparities, and sources of health information in U.S. older adults[J]. Orthop Nurs, 2018, 37(1): 54-65. DOI: 10.1097/nor.0000000000000418. [13] Suka, Odajima T, Okamoto M, et al. Relationship between health literacy, health information access, health behavior, and health status in Japanese people[J]. Patient Educ Couns, 2015, 98(5): 660-668. DOI: 10.1016/j.pec.2015.02.013. [14] Jeong SH, Kim HK. Health literacy and barriers to health information seeking: a nationwide survey in South Korea[J]. Patient Educ Couns, 2016, 99(11): 1880-1887. DOI: 10.1016/j.pec.2016.06.015. [15] 刘君, 刘春芳, 刘春晓, 等. 深圳口岸出入境人员疟疾相关知识态度和行为的研究[J]. 中国国境卫生检疫杂志, 2013, 36(1): 11-14. DOI: 10.16408/j.1004-9770.2013.01.019.Liu J, Liu CF, Liu CX, et al. Study of KABP on malaria among international travelers at Shenzhen Ports[J]. Chin J Front Heal Quar, 2013, 36(1): 11-14. DOI: 10.16408/j.1004-9770.2013.01.019. [16] 田睿, 谢铮, 李琼, 等. 驻加纳劳务人员疟疾行为干预效果评价[J]. 中国国境卫生检疫杂志, 2016, 39(3): 213-216. DOI: 10.16408/j.1004-9770.2016.03.018.Tian R, Xie Z, Li Q, et al. Evaluate the effect of the behavioral intervention of malaria on long-term workers in Ghana[J]. Chin J Front Heal Quar, 2016, 39(3): 213-216. DOI: 10.16408/j.1004-9770.2016.03.018. 期刊类型引用(4)
1. 刘海英,旷艳春,罗晓花. 驻湘基层部队官兵传染病健康素养及健康行为的现状调查. 当代护士(下旬刊). 2025(01): 107-111 .  百度学术
百度学术2. 杨秀琳,马宗康,马霞,马鑫. 东乡族自治县农村居民传染病健康素养调查. 预防医学. 2023(02): 166-170 . 百度学术3. 王婉菁,张兵,朱红兵. 经济活动与传染病的传播——基于流行性感冒的研究. 中国经济问题. 2023(06): 176-191 . 百度学术4. 郭艳军,孙静,李新萍. 住院老年患者骨质疏松健康素养水平及影响因素. 中国临床研究. 2022(06): 870-874 . 百度学术其他类型引用(4)
-


 下载:
下载:
 点击查看大图
点击查看大图
计量
- 文章访问数: 646
- HTML全文浏览量: 332
- PDF下载量: 65
- 被引次数: 8