

Diagnostic value of IP-10 in rheumatoid arthritis: a systematic review and Meta-analysis
-
摘要:
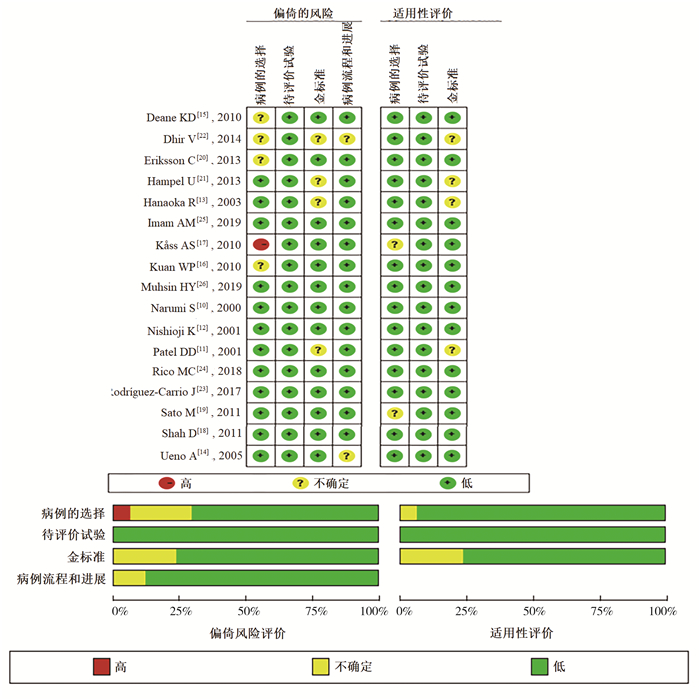
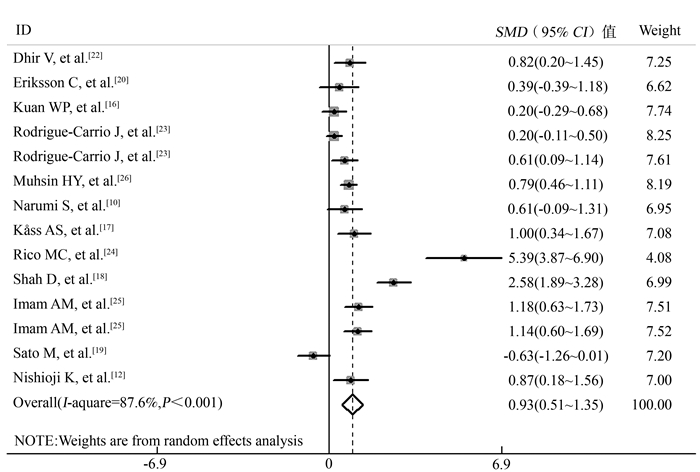
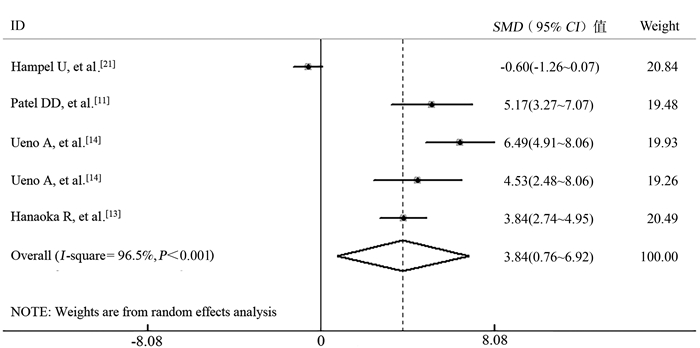
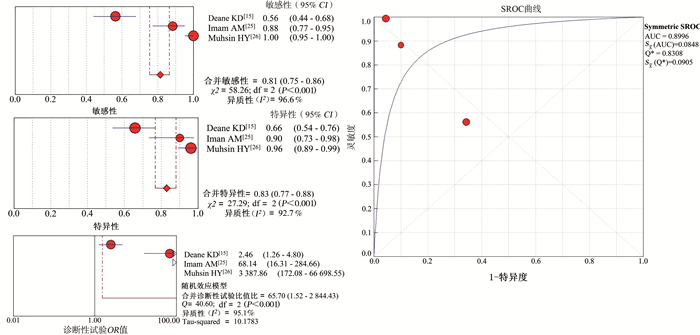
目的 分析类风湿关节炎(rheumatoid arthritis, RA)中干扰素诱导蛋白10(interferon-inducible protein 10, IP-10)表达水平的变化,评估其在RA中的诊断价值及与疾病活动的相关性。 方法 通过电子文献检索,在Cochrane图书馆、Scopus和PubMed数据库(截至2020年9月16日)搜索相关的文献,采用诊断准确性研究的质量评估工具2(quality assessment of diagnostic accuracy studies-2, QUADAS-2)对文献进行评价,并进行定量、综合分析。 结果 最终纳入文献17篇,RA患者IP-10表达水平高于健康对照(healthy control, HC)[标准化均数差(standard mean difference, SMD)=0.93, 95% CI : 0.51~1.35]。此外,IP-10表达水平在RA与骨关节炎(osteoarthritis, OA)中也存在差异(SMD=3.84, 95% CI: 0.76~6.92),但在RA和系统性红斑狼疮(systemic lupus erythematosus, SLE)之间差异无统计学意义。IP-10用于RA诊断的合并诊断比值比(diagnostic odds ratio, DOR)为65.70(95% CI: 1.52~2 844.43),曲线下面积(area under the curve, AUC)为0.889 6。 结论 IP-10表达水平在RA患者与HC和OA患者之间存在差异,可作为潜在的诊断性生物标志物。 Abstract:Objective We aimed to analyze the changes of interferon-inducible protein 10 (IP-10) in rheumatoid arthritis (RA) and evaluate the diagnostic value of IP-10 in RA and its correlation with disease activity. Methods We collected articles related to our research topic through an electronic literature search from the Cochrane Library, Scopus, and Pubmed (up to Sep16th, 2020). Quality assessment of diagnostic accuracy studies (QUADAS-2) tool was used to assess the quality of collected articles, and quantitative and comprehensive analysis was conducted. Results 17 studies were finally included in this study. IP-10 level in RA patients was higher than health controls [pooled standard mean difference (SMD) = 0.93, 95% CI= 0.51-1.35]. Besides, IP-10 levels in RA patients differed from osteoarthritis (OA) controls, with a pooled SMD and 95% CI being 3.84 (0.76-6.92). We found no significant difference in IP-10 levels between RA patients and systemic lupus erythematosus (SLE) controls. The pooled diagnostic odds ratio (DOR) value for IP-10 to diagnose RA was 65.70 (1.52-2 844.43) and AUC value was 0.899 6. Conclusion IP-10 levels differ from RA patients to HC and OA controls, it may be a potential diagnostic biomarker. -

图 2 QUADAS-2工具对合格文献的质量评价
Figure 2. Quality assessment of eligible literature by QUADAS-2 tool

图 3 12篇RA患者与HC的IP-10表达水平研究的Meta分析
Figure 3. Meta-analysis of 12 studies reporting the IP-10 level in RA compared with HC

图 4 关于RA与OA的IP-10表达水平的4篇文献Meta分析
Figure 4. Meta-analysis of 4 studies reporting the IP-10 level in RA compared with OA

图 5 IP-10试验用于诊断RA的敏感性、特异性、诊断比值比和受试者工作特征曲线森林图
Figure 5. Forest plots of pooled sensitivity, specificity, diagnostic odds ratio and summary receiver operating characteristic curve for IP-10 to diagnose RA
表 1 入选文献的特征描述
Table 1. Feature description of selected literature in research
第一作者(发表年份) 国家 RA HC SLE/OA 诊断标准 样本来源 检测方法 n 年龄(岁) a 女/男 病程(年) a n 年龄(岁) 女/男 n 年龄(岁) a 女/男 病程(年) a Narumi S [10], 2000 日本 12 38.0±10.0 10/2 NA 25 41.0±13.0 21/4 SLE: 28 b Ⅰ: 38.0±10.0 Ⅱ: 40.0±14.0 26/2 NA ACR 血清 ELISA Patel DD 11], 2001 美国 38 NA NA NA - - - - - - - NA 血清/滑膜组织 ELISA 10 NA NA NA - - - OA: 10 NA NA NA ELISA Nishioji K [12], 2001 日本 16 63.8±7.7 15/1 NA 20 46.4±14.4 10/10 - - - - ACR 血清 ELISA Hanaoka R [13], 2003 日本 32 NA NA NA - - - OA: 10 NA NA NA NA 滑膜液 ELISA Ueno A, [14] 2005 日本 20 58.5±12.3 17/3 8.5±6.7 - - - OA: 20 71.5±8.5 13/7 NA ACR 血清 & 滑膜液/滑膜组织 ELISA 10 64.7±9.9 8/2 24.1±7.7 - - - OA: 5 74.0±5.4 3/2 NA ELISA Deane KD [15], 2010 美国 73 39.1±8.4 30/43 NA 73 39.9±10.3 30/43 - - - - ACR 1987 血清 Bead-Based 14-Plex Assay Kuan WP, 2010 [16] 中国 28 49.0±13.0 26/2 7.3±6.0 40 38.0±9.0 39/1 - - - - ACR 1987 血清 Cytometric Bead Array Kåss AS [17], 2010 挪威 20 58.0 (34.0~79.0) 14/6 18.0 (0.3~49.0) 19 56.0 (32.0~79.0) 13/6 - - - - ACR 血清 Bead-Based Fluorescence Immunoassay Shah D [18], 2011 印度 30 24.2±10.4 25/5 4.5±1.5 30 26.7±5.4 27/3 SLE: 30 26.5±7.5 26/4 5.1±2.2 ACR 血清 ELISA Sato M, 2011 [19] 日本 20 60.1±3.2 19/1 10.4±1.9 20 NA NA - - - - ACR 1987 血清 ELISA Eriksson C [20], 2013 瑞典 21 53.4±14.2 6/3 < 1 9 53.2±4.9 6/3 SLE: 3 55.3±11.5 3/0 19.5 (0.5~45) ACR 血清 ELISA Hampel U [21], 2013 德国 16 64.2±12.8 16/5 NA - - - OA: 21 73.1±8.0 14/2 NA NA 滑膜液 9-Plex Chemokine array Dhir V [22], 2014 印度 36 NA NA NA 15 NA NA - - - - NA 血清 ELISA Rodríguez-Carrio J [23], 2017 西班牙 113 53.4 (22.0~87.0) 92/21 NA 113 53.8 (23.1~80.0) 82/31 - - - - ACR/EULAR 2010 血清 ELISA Rico MC [24], 2018 芬兰 20 51.0±8.2 95% NA 13 NA NA - - - - ACR 1987 血浆 Microarray by RCA Imam AM [25], 2019 埃及 60 c Ⅰ: 40.6±12.0 Ⅱ: 45.4±9.2 Ⅰ: 27/3; Ⅱ: 28/2 Ⅰ: 1.3±4.3 Ⅱ: 10.1±7.3 30 42.9±9.3 27/3 - - - - ACR/EULAR 2010 血清 ELISA Muhsin HY [26], 2019 伊拉克 77 46.8±13.2 54/23 NA 79 34.2±9.6 55/24 - - - - ACR/EULAR 2010 血清 ELISA 注:a以(x±s)和中位数(范围)表示数值; bⅠ组为活动期SLE组,Ⅱ组为非活动期SLE组,Ⅰ组为13例,Ⅱ组为15例; cⅠ组为早期RA组,Ⅱ组为长期RA组,两组分别为30例;NA:无法获取,原始文献数据不充分;ACR:美国风湿病学会;EULAR:欧洲风湿病防治联合会;-:原始文献无相应研究。  下载: 导出CSV
下载: 导出CSV
表 2 纳入研究的诊断性研究文献特征
Table 2. Characteristics of diagnostic studies included in the Meta-analysis
作者 年份 国家 RA HC 敏感度(%) 特异度(%) TP TN FP FN 年龄(x±s, 岁) n 年龄(x±s, 岁) n Deane KD [18] 2010 美国 40.00±10.30 73 39.90±10.30 73 56.2 65.8 41 48 25 32 Imam AM [25] 2019 埃及 ER: 40.60±11.99 LR: 45.43±9.17 60 42.87±9.31 30 88.3 90.0 53 27 3 7 Muhsin HY [26] 2019 伊拉克 46.80±13.20 77 34.20±9.60 79 100.0 96.2 77 76 3 0
下载: 导出CSV
表 3 RA和HC的IP-10表达水平亚组分析
Table 3. Subgroup analysis of IP-10 levels in RA and HC
分组 文献数量/研究分支 病人数量(n) SMD(95% CI)值 异质性检验 发表偏倚 I2(%) P值 t值 P值 总体 12/14 453 0.93(0.51~1.35) 87.6 < 0.001 2.11 0.056 样本大小 ≥30 5/6 287 1.08(0.51~1.64) 88.7 < 0.001 6.89 0.055 < 30 8/8 166 0.86(0.08~1.54) 87.8 < 0.001 7.67 0.036 年龄(岁) ≥50 6/7 218 0.74(0.07~1.41) 89.3 < 0.001 3.32 0.315 < 50 5/6 199 1.20(0.71~1.68) 78.5 < 0.001 4.37 0.142 地区 亚洲 4/5 219 0.74(0.13~1.35) 88.1 < 0.001 0.88 0.837 欧洲 7/7 174 1.25(0.31~2.18) 91.4 < 0.001 5.64 0.074 非洲 1/2 60 1.16(0.77~1.55) 注:发表偏倚使用Egger检验结果。
下载: 导出CSV
表 4 RA病例组和对照组的IP-10表达水平
Table 4. IP-10 level in RA and disease control group
文献数量/研究分支 病例数 SMD(95% CI)值 P值 异质性分析 发表偏倚b I2(%) P值 t值 P值 RA与OA的IP-10表达水平 总体 4/5 88 3.84(0.76~6.92) 0.015 96.5 < 0.001 16.26 < 0.001 滑膜液 3/3 68 3.20(-0.99~7.39) 0.134 97.8 < 0.001 16.26 0.102 滑膜组织 2/2 20 4.87(3.48~6.26) < 0.001 0.0 0.065 RA与SLE的IP-10表达水平a 2/3 42 -1.60(-3.36~0.15) 0.074 93.0 < 0.001 注:a两篇文献研究都使用的是血清标本;b发表偏倚采用Egger检验。
下载: 导出CSV
-
[1] Lloyd S, Bujkiewicz S, Wailoo AJ, et al. The effectiveness of anti-TNF-alpha therapies when used sequentially in rheumatoid arthritis patients: a systematic review and Meta-analysis[J]. Rheumatology (Oxford), 2010, 49: 2313-2321. DOI: 10.1093/rheumatology/keq169. [2] Luster AD. Chemokines--chemotactic cytokines that mediate inflammation[J]. Engl J Med, 1998, 338(7): 436-445. DOI: 10.1056/NEJM199802123380706. [3] Allen SJ, Crown SE. Chemokine: receptor structure, interactions, and antagonism[J]. Annu Rev Immunol, 2007, 25: 787-820. DOI: 10.1146/annurev.immunol.24.021605.090529. [4] Charo IF, Ransohoff RM. The many roles of chemokines and chemokine receptors in inflammation[J]. N Engl J Med, 2006, 354(6): 610-621. DOI: 10.1056/NEJMra052723. [5] Karin N, Razon H. Chemokines beyond chemo-attraction: CXCL10 and its significant role in cancer and autoimmunity[J]. Cytokine, 2018, 109: 24-28. DOI: 10.1016/j.cyto.2018.02.012. [6] Gasperini S, Marchi M, Calzetti F, et al. Gene expression and production of the monokine induced by IFN-gamma (MIG), IFN-inducible T cell alpha chemoattractant (I-TAC), and IFN-gamma-inducible protein-10 (IP-10) chemokines by human neutrophils[J]. J Immunol, 1999, 162(8): 4928-4937. http://www.ncbi.nlm.nih.gov/pubmed/10202039 [7] Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies[J]. Ann Intern Med, 2011, 155(8): 529-536. DOI: 10.7326/0003-4819-155-8-201110180-00009. [8] Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in Meta analyses[J]. BMJ, 2003, 327(7414): 557-560. DOI: 10.1136/bmj.327.7414.557. [9] Leeflang MM, Deeks JJ, Gatsonis C, et al. Systematic reviews of diagnostic test accuracy[J]. Ann Intern Med, 2008, 149(12): 889-897. DOI: 10.7326/0003-4819-149-12-200812160-00008. [10] Narumi S, Takeuchi T, Kobayashi Y, et al. Serum levels of ifn-inducible PROTEIN-10 relating to the activity of systemic lupus erythematosus[J]. Cytokine, 2000, 12(10): 1561-1565. DOI: 10.1006/cyto.2000.0757. [11] Patel DD, Zachariah JP, Whichard LP. CXCR3 and CCR5 Ligands in Rheumatoid Arthritis Synovium[J]. Clin Immunol, 2001, 98: 39-45. DOI: 10.1006/clim.2000.4957. [12] Nishioji K, Okanoue T, Itoh Y, et al. Increase of chemokine interferon-inducible protein-10 (IP-10) in the serum of patients with autoimmune liver diseases and increase of its mRNA expression in hepatocytes[J]. Clin Exp Immunol, 2001, 123(2): 271-279. DOI: 10.1046/j.1365-2249.2001.01391.x. [13] Hanaoka R, Kasama T, Muramatsu M, et al. A novel mechanism for the regulation of IFN-gamma inducible protein-10 expression in rheumatoid arthritis[J]. Arthritis Res Ther, 2003, 5(2): R74-81. DOI: 10.1186/ar616. [14] Ueno A, Yamamura M, Iwahashi M, et al. The production of CXCR3-agonistic chemokines by synovial fibroblasts from patients with rheumatoid arthritis[J]. Rheumatol Int, 2005, 25: 361-367. DOI: 10.1007/s00296-004-0449-x. [15] Deane KD, O'Donnell CI, Hueber W, et al. The number of elevated cytokines and chemokines in preclinical seropositive rheumatoid arthritis predicts time to diagnosis in an age-dependent manner[J]. Arthritis Rheum, 2010, 62(11): 3161-3172. DOI: 10.1002/art.27638. [16] Kuan WP, Tam LS, Wong CK, et al. CXCL 9 and CXCL 10 as Sensitive markers of disease activity in patients with rheumatoid arthritis[J]. J Rheumatol, 2010, 37(2): 257-264. DOI: 10.3899/jrheum.090769. [17] Kåss AS, Lea TE, Torjesen PA, et al. The association of luteinizing hormone and follicle-stimulating hormone with cytokines and markers of disease activity in rheumatoid arthritis: a case-control study[J]. Scand J Rheumatol, 2010, 39: 109-117. DOI: 10.3109/03009740903270607. [18] Shah D, Wanchu A, Bhatnagar A. Interaction between oxidative stress and chemokines: possible pathogenic role in systemic lupus erythematosus and rheumatoid arthritis[J]. Immunobiology, 2011, 216(9): 1010-1017. DOI: 10.1016/j.imbio.2011.04.001. [19] Sato M, Ohtsuka K, Takahashi R, et al. Involvement of CX3CL1/CX3CR1 axis in etanercept therapy for patients with active rheumatoid arthritis[J]. Open Access Rheumatol, 2011, 3: 1-7. DOI: 10.2147/OARRR.S16210. [20] Eriksson C, Rantapää-Dahlqvist S, Sundqvist KG, et al. Changes in chemokines and their receptors in blood during treatment with the TNF inhibitor infliximab in patients with rheumatoid arthritis[J]. Scand J Rheumatol, 2013, 42: 260-265. DOI: 10.3109/03009742.2012.754937. [21] Hampel U, Sesselmann S, Iserovich P, et al. Chemokine and cytokine levels in osteoarthritis and rheumatoid arthritis synovial fluid[J]. J Immunol Methods, 2013, 396(1-2): 134-139. DOI: 10.1016/j.jim.2013.08.007. [22] Dhir V, Sandhu A, Gupta N, et al. Change in CXCL10 on treatment with methotrexate similar to that reported with infliximab: comments on the article by Eriksson et al[J]. Scand J Rheumatol, 2014, 43(1): 83-84. DOI: 10.3109/03009742.2013.813961. [23] Rodríguez-Carrio J, Alperi-López M, López P, et al. High triglycerides and low high-density lipoprotein cholesterol lipid profile in rheumatoid arthritis: a potential link among inflammation, oxidative status, and dysfunctional high-density lipoprotein[J]. J Clin Lipidol, 2017, (11)4: 1043-1054. DOI: 10.1016/j.jacl.2017.05.009. [24] Rico MC, Manns JM, Driban JB, et al. Thrombospondin-1 and transforming growth factor beta are pro-inflammatory molecules in rheumatoid arthritis[J]. Transl Res, 2008, 152(2): 95-98. DOI: 10.1016/j.trsl.2008.06.002. [25] Imam AM, Hamed AM, Nasef SI, et al. Biochemical analysis of C-X-C motif chemokine ligand 10 (CXCL10) as a biomarker in patients with rheumatoid arthritis[J]. Egypt J Immunol, 2019, 26(2): 79-86. [26] Muhsin HY, Kadri ZHM, Ad'hiah AH, et al. Predictive significance of CXCL8, CXCL10 and CXCL16 in juvenile idiopathic and rheumatoid arthritis Iraqi patients[J]. Egyptian Rheumatologist, 2019. DOI: 10.1016/j.ejr.2019.06.002. [27] Puapatanakul P, Chansritrakul S, Susantitaphong P, et al. Interferon-inducible protein 10 and disease activity in systemic lupus erythematosus and lupus nephritis: a systematic review and Meta-analysis[J]. Int J Mol Sci, 2019, 20(19): 4954. DOI: 10.3390/ijms20194954. [28] Pandya JM, Lundell AC, Andersson K, et al. Blood chemokine profile in untreated early rheumatoid arthritis: CXCL10 as a disease activity marker[J]. Arthritis Res Ther, 2017, 19(1): 20. DOI: 10.1186/s13075-017-1224-1. [29] Chen DY, Shen GH, Chen YM, et al. Interferon-inducible protein-10 as a marker to detect latent and active tuberculosis in rheumatoid arthritis[J]. Int J Tuberc Lung Dis, 2011, 15(2): 192-200. http://www.ncbi.nlm.nih.gov/pubmed/21219680 [30] Ponce de Leon D, Acevedo-Vasquez E, Alvizuri S, et al. Comparison of an interferon-gamma assay with tuberculin skin testing for detection of tuberculosis (TB) infection in patients with rheumatoid arthritis in a TB-endemic population[J]. J Rheumatol, 2008, 35(5): 776-781. DOI: 10.1016/j.jbspin.2007.10.004. [31] Laragione T. Liver X receptor regulates rheumatoid arthritis fibroblast-like synoviocyte invasiveness, matrix Metalloproteinase 2 activation, interleukin-6 and CXCL10[J]. Mol Med, 2012, 18: 1009-1017. DOI: 10.2119/molmed.2012.00173. [32] Kasama T, Isojima S, Umemura M, et al. Serum macrophage migration inhibitory factor levels are correlated with response to tocilizumab therapy in patients with rheumatoid arthritis[J]. Rheumatol Int, 2014, 34(3): 429-433. DOI: 10.1007/s00296-013-2778-0. [33] Han BK, Kuzin I, Gaughan JP, et al. Baseline CXCL10 and CXCL13 levels are predictive biomarkers for tumor necrosis factor inhibitor therapy in patients with moderate to severe rheumatoid arthritis: a pilot, prospective study[J]. Arthritis Res Ther, 2016, 18: 93. DOI: 10.1186/s13075-016-0995-0. [34] Lasagni L, Francalanci M, Annunziato F, et al. An alternatively spliced variant of CXCR3 mediates the inhibition of endothelial cell growth induced by IP-10, Mig, and I-TAC, and acts as functional receptor for platelet factor 4[J]. J Exp Med, 2003, 197: 1537-1549. DOI: 10.1084/jem.20021897. [35] Muntyanu A, Abji F, Liang K, et al. Differential gene and protein expression of chemokines and cytokines in synovial fluid of patients with arthritis[J]. Arthritis Res Ther, 2016, 18(1): 296. DOI: 10.1186/s13075-016-1196-6. [36] Laragione T, Brenner M, Sherry B, et al. CXCL10 and its receptor CXCR3 regulate synovial fibroblast invasion in rheumatoid arthritis[J]. Arthritis Rheum, 2011, 63(11): 3274-3283. DOI: 10.1002/art.30573. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 347
- HTML全文浏览量: 214
- PDF下载量: 39
- 被引次数: 0