

Prevalence and associated factors of multimorbidity among newly reported HIV-positive individuals in Dehong Dai and Jingpo Autonomous Prefecture
-
摘要:
目的 了解云南省德宏傣族景颇族自治州(简称德宏州)新报告HIV感染者多共病患病率及其影响因素。 方法 2018年1月1日―2020年6月30日对德宏州新报告HIV感染者进行多共病的横断面研究。多共病指患有≥2种慢性疾病。 结果 共纳入468例HIV感染者,年龄35~ < 50岁者258例(55.1%),男女比约为1.4∶1,汉族者199例(42.5%)。多共病者共140例,患病率为29.9%,患有2、3、4、5和6种共病者分别占19.0%、8.3%、1.1%、0.9%和0.6%。患病率前5的共患疾病分别为血脂异常、慢性感染、高血压、贫血和肝纤维化,占比分别为48.9%、15.2%、13.9%、13.0%和8.3%。多因素Logistic回归分析模型分析结果显示,50~77岁年龄组(aOR=4.06, 95% CI: 1.98~8.33, P < 0.001)、曾经吸食或注射毒品(aOR=2.26, 95% CI: 1.23~4.14, P=0.009)和CD4+T淋巴细胞计数<200个/μl(aOR=2.03, 95% CI: 1.23~3.37, P=0.006)与多共病之间差异有统计学意义。 结论 德宏州新报告HIV感染者多共病率较高,尤其是年长、有毒品使用史和低CD4+T淋巴细胞计数水平者共病负担较高,提示HIV常规随访关怀中应考虑纳入多共病的综合监测与管理。 Abstract:Objective To explore the prevalence and associated factors of multimorbidity among the newly reported human immunodeficiency virus (HIV)-positive individuals in Dehong Dai Jingpo Autonomous Prefecture (Dehong). Methods From 1 January 2018 to 30 June 2020, a cross-sectional study was conducted to investigate the multimorbidity burden among newly reported HIV-positive individuals in Dehong. Multimorbidity was defined as the presence of at least two chronic diseases. Results 468 subjects were included, of which 258 (55.1%) were 35- < 50 years old, male to female ratio was about 1.4∶1 and 199 (42.5%) were Han Chinese. Among them, 140 (29.9%) had the multimorbidity. The prevalence of having two, three, four, five, six comorbidities were 19.0%, 8.3%, 1.1%, 0.9% and 0.6%, respectively. The top 5 comorbidities were dyslipidemia, chronic infections, hypertension, anemia and liver fibrosis, accounting for 48.9%, 15.2%, 13.9%, 13.0% and 8.3%, respectively. In multivariate Logistic regression, aged ≥ 50 years old (aOR=4.06, 95% CI: 1.98-8.33, P < 0.001), have history of drug abuse or injection drug use (aOR=2.26, 95% CI: 1.23-4.14, P=0.009) and CD4+T lymphocyte counts < 200 cells/μl (aOR=2.03, 95% CI: 1.23-3.37, P=0.006) were significantly associated with the presence of multimorbidity. Conclusions The prevalence of multimorbidity was high among newly reported HIV-positive individuals in Dehong particularly among the elderly, drug users and those with lower CD4 counts. Our data suggested that monitoring and managing multimorbidity should be integrated into regular HIV care. -
Key words:
- HIV /
- Multimorbidity /
- Cross-sectional study /
- Factors
-

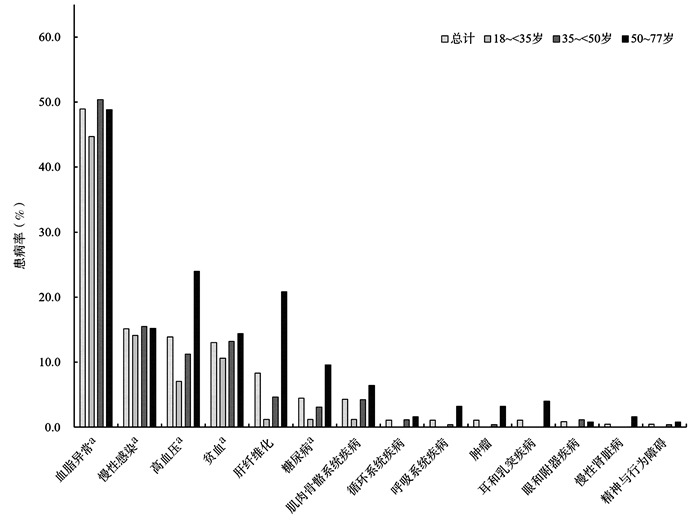
图 1 德宏州不同年龄段新报告HIV感染者各疾病患病率
注:a综合测量或生化检测和自我报告史定义。
Figure 1. Prevalence of comorbidities among newly reported HIV-positive individuals in Dehong Prefecture by age groups
表 1 德宏州新报告HIV感染者基本特征及多共病患病率[n(%)]
Table 1. Characteristics and prevalence of multimorbidity among newly reported HIV-positive individuals in Dehong Prefecture [n(%)]
特征 例数 多共病患病率 χ2值 P值 年龄(岁) 32.241 < 0.001 18~ < 35 85(18.2) 13(15.3) 35~ < 50 258(55.1) 66(25.6) 50~77 125(26.7) 61(48.8) 性别 9.322 0.002 男 271(57.9) 96(35.4) 女 197(42.1) 44(22.3) 文化程度 1.437 0.488 小学或文盲 248(53.0) 78(31.5) 初中 142(30.3) 43(30.3) 高中或中专及以上 78(16.7) 19(24.4) 民族 12.763 0.005 汉族 199(42.5) 77(38.7) 傣族 123(26.3) 29(23.6) 景颇族 105(22.4) 24(22.9) 其他 41(8.8) 10(24.4) BMI(kg/m2) 3.099 0.212 < 18.5 286(61.1) 83(29.0) 18.5~ < 24 61(13.0) 24(39.3) ≥24 121(25.9) 33(27.3) 经常体力劳动或锻炼(≥3次/周) 0.090 0.764 是 398(85.0) 118(29.7) 否 70(15.0) 22(31.4) 曾经饮酒 0.032 0.858 是 298(63.7) 90(30.2) 否 170(36.3) 50(29.4) 曾经吸烟 6.716 0.010 是 248(53.0) 87(35.1) 否 220(47.0) 53(24.1) 曾经吸食或注射毒品 9.035 0.003 是 74(15.8) 33(44.6) 否 394(84.2) 107(27.2) 感染途径 2.454 0.293 异性性传播 419(89.5) 130(31.0) 同性性传播 32(6.9) 7(21.9) 静脉吸毒 17(3.6) 3(17.7) WHO临床分期 12.947 0.005 Ⅰ期 260(55.6) 64(24.6) Ⅱ期 112(23.9) 34(30.4) Ⅲ期 59(12.6) 24(40.7) Ⅳ期 37(7.9) 18(48.7) CD4+T淋巴细胞计数(个/μl) 18.839 < 0.001 ≥350 215(45.9) 50(23.3) 200~ < 350 123(26.3) 32(26.0) < 200 130(27.8) 58(44.6) CD4+T淋巴细胞/CD8+T淋巴细胞比值a 5.357 0.069 < 0.4 319(69.7) 107(33.5) 0.4~ < 0.7 94(20.5) 23(24.5) ≥0.7 45(9.8) 9(20.0) 注:a表示数据有缺失。  下载: 导出CSV
下载: 导出CSV
表 2 德宏州新报告HIV感染者多共病的影响因素分析
Table 2. Factors associated with multimorbidity among newly reported HIV-positive individuals in Dehong Prefecture
特征 单因素分析 多因素分析 OR (95% CI)值 P值 aOR (95% CI)值 P值 年龄(岁) 18~ < 35 1.00 1.00 35~ < 50 1.90 (0.99~3.66) 0.054 1.43 (0.73~2.83) 0.299 50~77 5.28 (2.66~10.49) < 0.001 4.06 (1.98~8.33) < 0.001 性别 男 1.00 1.00 女 0.52 (0.35~0.80) 0.002 0.64 (0.32~1.25) 0.188 文化程度 小学或文盲 1.00 初中 0.95 (0.61~1.48) 0.810 高中或中专及以上 0.70 (0.39~1.26) 0.234 民族 汉族 1.00 1.00 傣族 0.49 (0.30~0.81) 0.005 0.58 (0.34~1.01) 0.054 景颇族 0.47 (0.27~0.80) 0.006 0.56 (0.31~1.02) 0.057 其他 0.51 (0.24~1.10) 0.087 0.56 (0.24~1.28) 0.168 BMI(kg/m2) < 18.5 1.00 18.5~ < 24 1.59 (0.89~2.82) 0.115 ≥24 0.92 (0.57~1.47) 0.721 经常体力劳动或锻炼 0.92 (0.53~1.59) 0.764 曾经饮酒 1.04 (0.69~1.57) 0.858 曾经吸烟 1.70 (1.14~2.55) 0.010 0.91 (0.47~1.76) 0.771 曾经吸食或注射毒品 2.16 (1.30~3.59) 0.003 2.26 (1.23~4.14) 0.009 感染途径 异性性传播 1.00 同性性传播 0.62 (0.26~1.48) 0.282 静脉吸毒 0.48 (0.14~1.69) 0.250 WHO临床分期 Ⅰ期 1.00 Ⅱ期 1.34 (0.82~2.18) 0.250 Ⅲ期 2.10 (1.16~3.79) 0.014 Ⅳ期 2.90 (1.44~5.86) 0.003 CD4+T淋巴细胞计数(个/μl) ≥350 1.00 1.00 200~ < 350 1.16 (0.70~1.94) 0.570 0.97 (0.56~1.69) 0.926 < 200 2.66 (1.66~4.25) < 0.001 2.03 (1.23~3.37) 0.006 CD4+T淋巴细胞/CD8+T淋巴细胞比值a < 0.4 1.00 0.4~ < 0.7 0.64 (0.38~1.08) 0.098 ≥0.7 0.50 (0.23~1.07) 0.072 注:a表示数据有缺失。
下载: 导出CSV
-
[1] Trickey A, May MT, Vehreschild JJ, et al. Survival of HIV-positive patients starting antiretroviral therapy between 1996 and 2013: a collaborative analysis of cohort studies[J]. Lancet HIV, 2017, 4(8): e349-e356. DOI: 10.1016/s2352-3018(17)30066-8. [2] Gueler A, Moser A, Calmy A, et al. Life expectancy in HIV-positive persons in Switzerland: matched comparison with general population[J]. AIDS, 2017, 31(3): 427-436. DOI: 10.1097/qad.0000000000001335. [3] Samji H, Cescon A, Hogg RS, et al. Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada[J]. PLoS One, 2013, 8(12): e81355. DOI: 10.1371/journal.pone.0081355. [4] Guaraldi G, Orlando G, Zona S, et al. Premature age-related comorbidities among HIV-infected persons compared with the general population[J]. Clin Infect Dis, 2011, 53(11): 1120-1126. DOI: 10.1093/cid/cir627. [5] Pathai S, Bajillan H, Landay AL, et al. Is HIV a model of accelerated or accentuated aging?[J]. J Gerontol A Biol Sci Med Sci, 2014, 69(7): 833-842. DOI: 10.1093/gerona/glt168. [6] Althoff KN, Smit M, Reiss P, et al. HIV and ageing: improving quantity and quality of life[J]. Curr Opin HIV AIDS, 2016, 11(5): 527-536. DOI: 10.1097/coh.0000000000000305. [7] Thienemann F, Sliwa K, Rockstroh JK. HIV and the heart: the impact of antiretroviral therapy: a global perspective[J]. Eur Heart J, 2013, 34(46): 3538-3546. DOI: 10.1093/eurheartj/eht388. [8] Non LR, Escota GV, Powderly WG. HIV and its relationship to insulin resistance and lipid abnormalities[J]. Transl Res, 2017, 183: 41-56. DOI: 10.1016/j.trsl.2016.12.007. [9] Schank M, Zhao J, Moorman JP, et al. The impact of HIV- and ART-induced mitochondrial dysfunction in cellular senescence and aging[J]. Cells, 2021, 10(1): 174. DOI: 10.3390/cells10010174. [10] Lagathu C, Bereziat V, Gorwood J, et al. Metabolic complications affecting adipose tissue, lipid and glucose metabolism associated with HIV antiretroviral treatment[J]. Expert Opin Drug Saf, 2019, 18(9): 829-840. DOI: 10.1080/14740338.2019.1644317. [11] Kingery JR, Alfred Y, Smart LR, et al. Short-term and long-term cardiovascular risk, metabolic syndrome and HIV in Tanzania[J]. Heart, 2016, 102(15): 1200-1205. DOI: 10.1136/heartjnl-2015-309026. [12] Nduka CU, Stranges S, Kimani PK, et al. Is there sufficient evidence for a causal association between antiretroviral therapy and diabetes in HIV-infected patients? A meta-analysis[J]. Diabetes Metab Res Rev, 2017, 33(6). DOI: 10.1002/dmrr.2902. [13] Back D, Marzolini C. The challenge of HIV treatment in an era of polypharmacy[J]. J Int AIDS Soc, 2020, 23(2): e25449. DOI: 10.1002/jia2.25449. [14] 中国高血压防治指南修订委员会. 中国高血压防治指南(2018年修订版)[J]. 中国心血管杂志, 2019, 24(1): 24-56. DOI: 10.3969/j.issn.1007-5410.2019.01.002.Writing Group of Chinese Guidelines for the Management of Hypertension. 2018 Chinese guidelines for the management of hypertension[J]. Chin J Cardiovasc Med, 2019, 24(1): 24-56. DOI: 10.3969/j.issn.1007-5410.2019.01.002. [15] 中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2020年版)[J]. 中华糖尿病杂志, 2021, 13(4): 315-409. DOI: 10.3760/cma.j.cn115791-20210221-00095.Chinese Diabetes Society. Guidelines for the prevention and control of type 2 diabetes in China (2020 Edition)[J]. Chin J Diabetes Mellitus, 2021, 13(4): 315-409. DOI: 10.3760/cma.j.cn115791-20210221-00095. [16] 中华医学会, 中华医学会杂志社, 中华医学会全科医学分会, 等. 血脂异常基层诊疗指南(2019年)[J]. 中华全科医师杂志, 2019, 18(5): 406-416. DOI: 10.3760/cma.j.issn.1671-7368.2019.05.003.Chinese Medical Association, Chinese Medical Journals Publishing House, Chinese Society of General Practice, et al. Guideline for primary care of dysliplidemias (2019)[J]. Chin J Gen Pract, 2019, 18(5): 406-416. DOI: 10.3760/cma.j.issn.1671-7368.2019.05.003. [17] 中华医学会肝病学分会, 中华医学会感染病学分会. 丙型肝炎防治指南(2019年版)[J]. 中华传染病杂志, 2020, 38(1): 9-28. DOI: 10.3760/cma.j.issn.1000-6680.2020.01.004.Chinese Society of Hepatology, Chinese Society of Infectious Diseases. Guidelines for the prevention and treatment of hepatitis C (2019 version)[J]. Chin J Infect Dis, 2020, 38(1): 9-28. DOI: 10.3760/cma.j.issn.1000-6680.2020.01.004. [18] Shen YZ, Wang ZY, Lu HZ, et al. Prevalence of anemia among adults with newly diagnosed HIV/AIDS in China[J]. PLoS One, 2013, 8(9): e73807. DOI: 10.1371/journal.pone.0073807. [19] Zhang LX, Wang F, Wang L, et al. Prevalence of chronic kidney disease in China: a cross-sectional survey[J]. Lancet, 2012, 379(9818): 815-822. DOI: 10.1016/s0140-6736(12)60033-6. [20] 上海慢性肾脏病早发现及规范化诊治与示范项目专家组. 慢性肾脏病筛查诊断及防治指南[J]. 中国实用内科杂志, 2017, 37(1): 28-34. DOI: 10.19538/j.nk2017010108.Shanghai Expert Group of Early Detection, Standardized Diagnosis, Treatment and Demonstration Project of Chronic Kidney Disease. Guidelines for screening, diagnosis and prevention of chronic kidney disease[J]. Chin J Pract Intern Med, 2017, 37(1): 28-34. DOI: 10.19538/j.nk2017010108. [21] Chen R, Chen J, Tang Q, et al. Use of comedications and potential drug -drug interactions in people living with HIV in China[J]. J Infection Chemother, 2020, 26(7): 722-728. DOI: 10.1016/j.jiac.2020.04.003. [22] Schouten J, Wit FW, Stolte IG, et al. Cross-sectional comparison of the prevalence of age-associated comorbidities and their risk factors between HIV-infected and uninfected individuals: the AGEhIV cohort study[J]. Clin Infect Dis, 2014, 59(12): 1787-1797. DOI: 10.1093/cid/ciu701. [23] Lin L, Li TS. Multidisciplinary collaborative integrated management of increasingly prominent HIV complications in the post-cART era[J]. HIV Med, 2020, 21(11): 683-691. DOI: 10.1111/hiv.13022. [24] Abebe F, Schneider M, Asrat B, et al. Multimorbidity of chronic non-communicable diseases in low- and middle-income countries: a scoping review[J]. J Comorb, 2020, 10: 2235042x20961919. DOI: 10.1177/2235042x20961919. [25] Pacheco YM, Jarrin I, Rosado I, et al. Increased risk of non-AIDS-related events in HIV subjects with persistent low CD4 counts despite cART in the CoRIS cohort[J]. Antiviral Research, 2015, 117: 69-74. DOI: 10.1016/j.antiviral.2015.03.002. [26] 徐小慧, 单淑晴, 时允, 等. 云南省德宏州接受抗病毒治疗的HIV感染者高血压患病率及其影响因素[J]. 中国初级卫生保健, 2020, 34(4): 48-51. DOI: 10.3969/j.issn.1001-568x.2020.04.0015.Xu XH, Shan SQ, Shi Y, et al. Prevalence and associated factors of hypertension among HIV-infected individuals receiving combination antiretroviral therapy in Dehong Prefecture, Yunnan Province[J]. Chin Primary Health Care, 2020, 34(4): 48-51. DOI: 10.3969/j.issn.1001-568x.2020.04.0015. [27] 叶润华, 李静, 姚仕堂, 等. 德宏傣族景颇族自治州抗病毒治疗的HIV/AIDS糖尿病患病率及其相关因素分析[J]. 中华流行病学杂志, 2019, 40(6): 654-659. DOI: 10.3760/cma.j.issn.0254-6450.2019.06.010.Ye RH, Li J, Yao ST, et al. Prevalence and related factors on diabetes among HIV/AIDS receiving antiretroviral therapy in Dehong Dai and Jingpo Autonomous Prefecture[J]. Chin J Epidemiol, 2019, 40(6): 654-659. DOI: 10.3760/cma.j.issn.0254-6450.2019.06.010. [28] 姚仕堂, 何春燕, 曹东冬, 等. 德宏傣族景颇族自治州2010-2019年HIV感染者抗病毒治疗后艾滋病和非艾滋病相关死亡及其影响因素分析[J]. 中华流行病学杂志, 2021, 42(4): 632-637. DOI: 10.3760/cma.j.cn112338-20200903-01121.Yao ST, He CY, Cao DD, et al. Incidence and influencing factors of AIDS-related and non-AIDS-related deaths after receiving antiretroviral therapy among HIV-positive individuals in Dehong Dai and Jingpo Autonomous Prefecture, 2010-2019[J]. Chin J Epidemiol, 2021, 42(4): 632-637. DOI: 10.3760/cma.j.cn112338-20200903-01121. [29] 王继宝, 陈晓晨, 段星, 等. 云南省德宏州2016-2017年新报告中国和缅甸籍HIV感染者中HCV的流行病学特征[J]. 中华疾病控制杂志, 2019, 23(10): 1293-1296, 1300. DOI: 10.16462/j.cnki.zhjbkz.2019.10.026.Wang JB, Chen XC, Duan X, et al. Epidemiological characteristics of co-infection of hepatitis C virus among newly reported HIV infected patients in Chinese and Burmese from 2016 to 2017 in Dehong Prefecture of Yunnan Province[J]. Chin J Dis Control Prev, 2019, 23(10): 1293-1296, 1300. DOI: 10.16462/j.cnki.zhjbkz.2019.10.026. [30] Shen Y, Wang J, Wang Z, et al. Prevalence of dyslipidemia among antiretroviral-naive HIV-infected individuals in China[J]. Medicine, 2015, 94(48): e2201. DOI: 10.1097/md.0000000000002201. [31] De FD, Verboeket SO, Underwood J, et al. Patterns of co-occurring comorbidities in people living with HIV[J]. Open Forum Infect Dis, 2018, 5(11): ofy272. DOI: 10.1093/ofid/ofy272. [32] Yang X, Zhang J, Chen S, et al. Comorbidity patterns among people living with HIV: a hierarchical clustering approach through integrated electronic health records data in South Carolina[J]. AIDS Care, 2021, 33(5): 594-606. DOI: 10.1080/09540121.2020.1844864. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 433
- HTML全文浏览量: 308
- PDF下载量: 63
- 被引次数: 0