

Prognostic factors and nomogram construction of non-small cell lung cancer patients based on inflammatory and nutritional indicators
-
摘要:
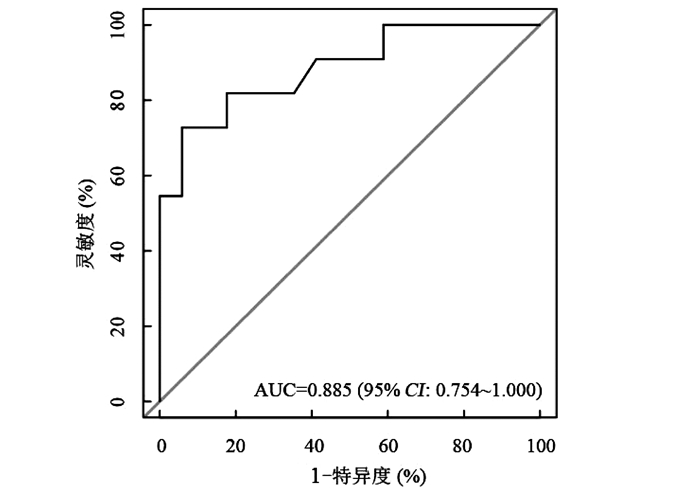
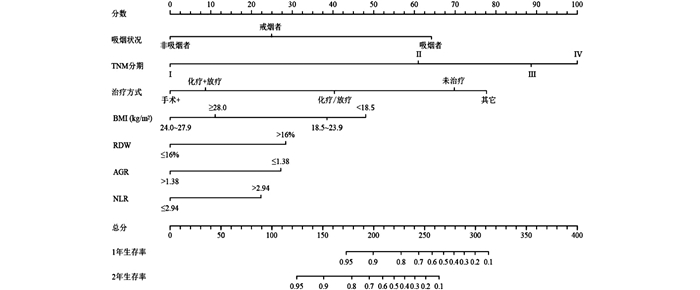
目的 基于炎症和营养指标探讨非小细胞肺癌(non-small-cell lung cancer, NSCLC)患者预后的影响因素建立预测总生存期(overall survival, OS)的列线图。 方法 选取苏州肺癌生存队列2016年1月-2020年1月NSCLC患者371例,随机分为训练队列(n=278)和验证队列(n=93)。在训练队列中,通过Cox比例风险模型确定独立危险因素,构建列线图。通过Bootstrap法和十折交叉验证对模型的性能进行评价。 结果 训练队列和验证队列的1年生存率分别为83.8%和83.9%,2年生存率分别为65.1%和66.7%。最后纳入模型的变量为吸烟状况、分期、治疗方式、BMI、红细胞分布宽度(red cell distribution width, RDW)、中性粒细胞与淋巴细胞比值(neutrophil-to-lymphocyte ratio, NLR)和白蛋白与球蛋白比值(albumin-to-globulin ratio, AGR)(均有P < 0.05)。训练队列和验证队列的预测OS的C-index分别为0.824和0.762,模型十折交叉验证的平均准确率为77.3%,ROC曲线下面积(area under the curve, AUC)为0.885(95% CI: 0.751~1.000)。 结论 基于炎症和营养指标构建的列线图可以有效地预测NSCLC患者的总生存期。 Abstract:Objective To explore the prognostic factors of non-small-cell lung cancer (NSCLC) patients based on inflammation and nutritional indicators, and to establish a nomogram for predicting overall survival (OS). Methods A total of 371 NSCLC patients in Suzhou lung cancer survival cohort from January 2016 to January 2020 were randomly divided into a training cohort (n=278) and a validation cohort (n=93). In the training cohort, independent risk factors were determined by Cox proportional hazard model and a nomogram was constructed. The bootstrap and ten-fold cross-validation were used to evaluate the performance of the model. Results The 1-year survival rate was 83.8% in the training cohort and 83.9% in the validation cohort, and the 2-year survival rate was 65.1% and 66.7%, respectively. Finally, the variables included in the model were smoking, stage, treatment, body mass index (BMI), red blood cell distribution width (RDW), neutrophil-to-lymphocyte ratio (NLR), and albumin-to-globulin ratio (AGR) as risk factors for OS of NSCLC patients (P < 0.05). The C-index of the training cohort and validation cohort for predicting OS were 0.824 and 0.762, respectively. After ten-fold cross-validation of the model, its average accuracy rate was 77.3%, and the area under the curve (AUC) was 0.885 (95% CI: 0.751-1.000). Conclusions The nomogram based on inflammation and nutrition indicators can effectively predict OS of NSCLC patients. -
Key words:
- Inflammation /
- Nutrition /
- Non-small cell lung cancer /
- Nomogram
-

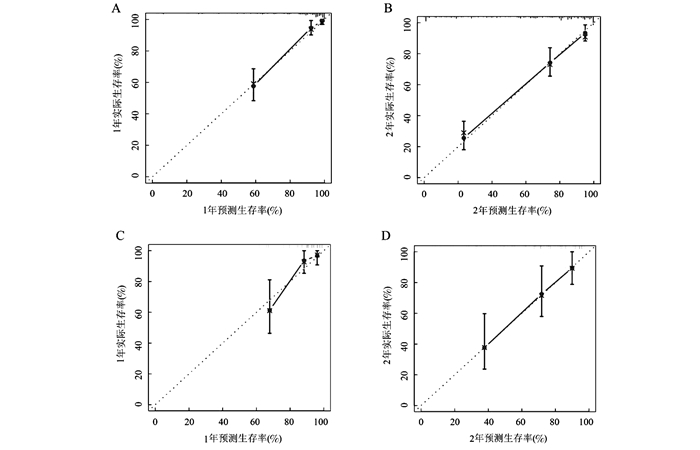
图 2 训练队列(A, B)和验证队列(C, D)1年和2年生存率的校准曲线
Figure 2. The calibration curve for the 1-year OS and 2-year OS in training cohort and validation cohort
表 1 训练队列与验证队列中患者的临床特征比较[n(%)]
Table 1. Comparison of clinical characteristics of patients in training cohort and validation cohort [n(%)]
变量 训练队列
(n=278)验证队列
(n=93)χ2/Z值 P值 变量 训练队列
(n=278)验证队列
(n=93)χ2/Z值 P值 年龄(岁) 0.666 0.466 中性粒细胞(109/L) 2.689 0.101 ≤65 160 58 ≤6.3 228(82.0) 83(89.2) >65 118 35 >6.3 50(18.0) 10(10.8) 性别 0.335 0.622 淋巴细胞(109/L) 0.022 0.882 男 170(61.2) 60(64.5) ≤1.1 89(32.0) 29(31.2) 女 108(38.8) 33(35.5) >1.1 189(68.0) 64(68.8) BMI(kg/m2) 1.097 0.272 血小板(109/L) 0.238 0.625 < 18.5 27(9.7) 9(9.7) ≤350 246(88.5) 84(90.3) 18.5~ < 24.0 183(65.8) 54(58) >350 32(11.5) 9(9.7) 24.0~ < 28.0 45(16.2) 22(23.7) C-反应蛋白(g/L) 0.166 0.683 ≥28.0 23(8.3) 8(8.6) ≤3 50(18.0) 15(16.1) 慢性阻塞性肺病 0.900 0.383 >3 228(82.0) 78(83.9) 有 12(4.3) 2(2.2) 球蛋白(g/L) 1.175 0.278 无 266(95.7) 91(97.8) ≤30 174(62.6) 64(68.8) 肿瘤家族史 0.179 0.728 >30 104(37.4) 29(31.2) 有 37(13.3) 14(15.1) 白蛋白(g/L) 0.742 0.389 无 241(86.7) 79(84.9) ≤35 43(15.5) 11(11.8) 吸烟状况 0.564 0.756 >35 235(84.5) 82(88.2) 非吸烟者 139(50.0) 43(46.2) 血红蛋白(g/L) 0.999 0.318 戒烟者 71(25.5) 27(29.1) ≤120 118(42.4) 34(36.6) 吸烟者 68(24.5) 23(24.7) >120 160(57.6) 59(63.4) 饮酒状况 0.726 0.449 RDW(%) 0.356 0.837 有 61(21.9) 24(25.8) ≤16 237(85.3) 79(84.9) 无 217(78.1) 69(74.2) >16 40(14.4) 14(15.1) 肿瘤分型 1.179 0.588 PLR 1.250 0.263 腺癌 183(65.8) 63(67.7) ≤147 119(42.8) 46(49.5) 鳞癌 74(26.6) 26(28.0) >147 159(57.2) 47(50.5) 其他 21(7.6) 4(4.3) NLR 1.993 0.158 TNM分期 0.470 0.638 ≤2.94 147(52.9) 57(61.3) Ⅰ 37(13.3) 13(14) >2.94 131(47.1) 36(38.4) Ⅱ 22(7.9) 9(9.7) SII 1.512 0.219 Ⅲ 63(22.7) 17(18.3) ≤867 181(65.1) 67(72.0) Ⅳ 156(56.1) 54(58.0) >867 97(34.9) 26(28.0) 治疗方式 3.007 0.556 PNI 0.074 0.786 未治疗 16(5.8) 5(5.4) ≤48.5 148(53.2) 48(51.6) 手术+ a 115(41.4) 48(51.6) >48.5 130(46.8) 45(48.4) 化疗或放疗 112(40.2) 30(32.3) AGR 0.120 0.729 化疗+放疗 27(9.7) 8(8.5) ≤1.38 105(37.8) 37(39.8) 其他 8(2.9) 2(2.2) >1.38 173(62.2) 56(60.2) 白细胞(109/L) 0.101 0.751 ≤10 251(90.3) 85(91.4) >10 27(9.7) 8(8.6%) 注:a手术+:仅手术或手术与辅助治疗。  下载: 导出CSV
下载: 导出CSV
表 2 NSCLC患者总生存期的单因素和多因素分析
Table 2. Univariate and multivariate analysis of OS for NSCLC patients
变量 单因素分析 多因素分析 HR(95% CI)值 P值 HR(95% CI)值 P值 年龄(≤65为对照) 1.048(0.701~1.565) 0.821 0.428 性别(男为对照) 0.348(0.215~0.565) < 0.001 0.098 BMI(< 18.5 kg/m2为对照) 0.041 0.017 18.5~<24.0 0.806(0.437~1.486) 0.489 0.775(0.399~1.504) 0.451 24.0~<28.0 0.352(0.148~0.836) 0.018 0.279(0.110~0.704) 0.007 ≥28.0 0.413(0.145~1.172) 0.096 0.389(0.127~1.195) 0.099 慢性阻塞性肺病(有为对照) 1.011(0.372~2.752) 0.982 0.936 肿瘤家族史(有为对照) 1.580(0.796~3.138) 0.191 0.135 吸烟状况(非吸烟者为对照) < 0.001 < 0.001 戒烟者 1.864(1.080~3.215) 0.025 1.946(1.101~3.438) 0.022 吸烟者 5.192(3.229~8.350) < 0.001 5.528(3.325~9.193) < 0.001 饮酒(有为对照) 0.656(0.420~1.023) 0.063 0.517 肿瘤分型(腺癌为对照) 0.039 0.919 鳞癌 1.745(1.134~2.685) 0.011 0.929 其他 1.338(0.638~2.807) 0.441 0.681 TNM分期(Ⅰ为对照) < 0.001 0.019 Ⅱ 5.607(0.583~53.911) 0.135 5.013(0.488~51.514) 0.175 Ⅲ 11.715(1.559~88.035) 0.017 10.387(1.299~83.035) 0.027 Ⅳ 23.580(3.278~169.606) 0.002 14.244(1.873~108.303) 0.010 治疗方式(未治疗为对照) < 0.001 < 0.001 手术+a 0.119(0.056~0.249) < 0.001 0.151(0.066~0.345) < 0.001 化疗或放疗 0.473(0.252~0.886) 0.019 0.445(0.222~0.890) 0.022 化疗+放疗 0.308(0.130~0.733) 0.008 0.195(0.075~0.506) 0.001 其他 0.875(0.328~2.332) 0.789 1.178(0.409~3.394) 0.762 白细胞(≤10×109/L为对照) 2.372(1.367~4.116) 0.002 0.100 中性粒细胞(≤6.3×109/L为对照) 1.930(1.224~3.044) 0.005 0.475 淋巴细胞(≤1.1×109/L为对照) 0.884(0.581~1.345) 0.564 0.281 血小板(≤350×109/L为对照) 3.820(2.397~6.088) < 0.001 0.096 C-反应蛋白(≤3 mg/L为对照) 2.817(1.366~5.809) 0.005 0.195 球蛋白(≤30 g/L为对照) 1.844(1.238~2.747) 0.003 0.492 白蛋白(≤35 g/L为对照 0.455(0.285~0.727) 0.001 0.404 血红蛋白(≤120 g/L为对照) 0.449(0.301~0.670) < 0.001 0.495 RDW(≤16%为对照) 2.174(1.339~3.528) 0.002 2.155(1.273~3.648) 0.004 PLR(≤147为对照) 2.624(1.673~4.116) < 0.001 0.728 NLR(≤2.94为对照) 2.067(1.377~3.104) < 0.001 1.812(1.141~2.878) 0.012 SII(≤867为对照) 2.622(1.758~3.909) < 0.001 0.473 PNI(≤48.5为对照) 0.399(0.259~0.615) < 0.001 0.310 AGR(≤1.38为对照) 0.370(0.248~0.553) < 0.001 0.495(0.320~0.763) 0.001 注:a手术+:仅手术或手术与辅助治疗。
下载: 导出CSV
表 3 腺癌和鳞癌患者的多因素分析
Table 3. Multivariate analysis of patients with adenocarcinoma and squamous cell carcinoma
变量 HR(95% CI)值 P值 变量 HR(95% CI)值 P值 腺癌 鳞癌 吸烟状况(非吸烟者为对照) < 0.001 BMI(< 18.5 kg/m2为对照) 0.022 戒烟者 2.201(1.026~4.720) 0.043 18.5~<24.0 0.146(0.040~0.531) 0.003 吸烟者 7.013(3.238~15.187) < 0.001 24.0~<28.0 0.073(0.007~0.740) 0.027 治疗方式(未治疗为对照) 0.010 ≥28.0 0.050(0.000~6.907) 0.970 手术+a 0.238(0.082~0.688) 0.008 TNM分期(Ⅰ为对照) 0.032 化疗或放疗 0.770(0.323~1.836) 0.556 Ⅱ 44.340(1.342~126.037) 0.034 化疗+放疗 0.414(0.112~1.523) 0.184 Ⅲ 8.899(0.509~155.493) 0.134 其他 2.099(0.532~8.282) 0.290 Ⅳ 20.551(1.249~338.122) 0.034 RDW(≤16%为对照) 2.942(1.472~5.879) 0.002 AGR(≤1.38为对照) 0.399(0.165~0.969) 0.042 NLR(≤2.94为对照) 2.045(1.156~3.616) 0.014 PNI(≤48.5为对照) 0.170(0.046~0.620) 0.007 血小板(≤350×109/L为对照) 2.492(1.184~5.246) 0.016 注:a手术+:仅手术或手术与辅助治疗。
下载: 导出CSV
-
[1] Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012[J]. Int J Cancer, 2015, 136(5): E359-E386. DOI: 10.1002/ijc.29210. [2] Xie D, Allen MS, Marks R, et al. Nomogram prediction of overall survival for patients with non-small-cell lung cancer incorporating pretreatment peripheral blood markers [J]. Eur J Cardio- Thorac Surg, 2018, 53(6): 1214-1222. DOI: 10.1093/ejcts/ezx462. [3] Cagini L, Monacelli M, Giustozzi G, et al. Biological prognostic factors for early stage completely resected non-small cell lung cancer [J]. J Surg Oncol, 2000, 74(1): 53-60. DOI:10.1002/1096-9098(200005)74:1<53::aid-jso13>3.0.co;2-d. [4] Hoang T, Xu R, Schiller JH, et al. Clinical model to predict survival in chemonaive patients with advanced non-small-cell lung cancer treated with third-generation chemotherapy regimens based on eastern cooperative oncology group data [J]. J Clin Oncol, 2005, 23(1): 175-183. DOI: 10.1200/JCO.2005.04.177. [5] Guo M, Li W, Li B, et al. Prognostic value of delta inflammatory biomarker-based nomograms in patients with inoperable locally advanced NSCLC [J]. Int Immunopharmacol, 2019, 72(440): 395-401. DOI: 10.1016/j.intimp.2019.04.032. [6] Guo M, Li B, Yu Y, et al. Delineating the pattern of treatment for elderly locally advanced NSCLC and predicting outcomes by a validated model: A SEER based analysis [J]. Cancer Med, 2019, 8(5): 2587-2598. DOI: 10.1002/cam4.2127. [7] Kang J, Ning MS, Feng H, et al. Predicting 5-year progression and survival outcomes for early stage non-small cell lung cancer treated with stereotactic ablative radiation therapy: development and validation of robust prognostic nomograms [J]. Int J Radiat Oncol Biol Phys, 2020, 106(1): 90-99. DOI: 10.1016/j.ijrobp.2019.09.037. [8] Kusumanto YH, Dam WA, Hospers GA, et al. Platelets and granulocytes, in particular the neutrophils, form important compartments for circulating vascular endothelial growth factor [J]. Angiogenesis, 2003, 6(4): 283-287. DOI: 10.1023/B:AGEN.0000029415.62384.ba. [9] Wang Y, Qu X, Kam NW, et al. An inflammation-related nomogram for predicting the survival of patients with non-small cell lung cancer after pulmonary lobectomy [J]. BMC Cancer, 2018, 18(1): 692. DOI: 10.1186/s12885-018-4513-4. [10] Shepshelovich D, Xu W, Lu L, et al. Body Mass Index (BMI), BMI change, and overall survival in patients with SCLC and NSCLC: a pooled analysis of the international lung cancer consortium [J]. J Thorac Oncol, 2019, 14(9): 1594-1607. DOI: 10.1016/j.jtho.2019.05.031. [11] Laky B, Janda M, Bauer J, et al. Malnutrition among gynaecological cancer patients [J]. Eur J Clin Nutr, 2007, 61(5): 642-646. DOI: 10.1038/sj.ejcn.1602540. [12] He J, Pan H, Liang W, et al. Prognostic effect of albumin-to-globulin ratio in patients with solid tumors: a systematic review and meta-analysis [J]. J Cancer, 2017, 8(19): 4002-4010. DOI: 10.7150/jca.21141. [13] Zhang H, Zhang B, Zhu K, et al. Preoperative albumin-to-globulin ratio predicts survival in patients with non-small-cell lung cancer after surgery [J]. J Cell Physiol, 2019, 234(3): 2471-2479. DOI: 10.1002/jcp.26766. [14] Koma Y, Onishi A, Matsuoka H, et al. Increased red blood cell distribution width associates with cancer stage and prognosis in patients with lung cancer [J]. PLoS One, 2013, 8(11): e80240. DOI: 10.1371/journal.pone.0080240. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 362
- HTML全文浏览量: 182
- PDF下载量: 59
- 被引次数: 0