

Analysis of the trend of total delay among pulmonary tuberculosis patients with positive etiology in Yunnan Province
-
摘要:
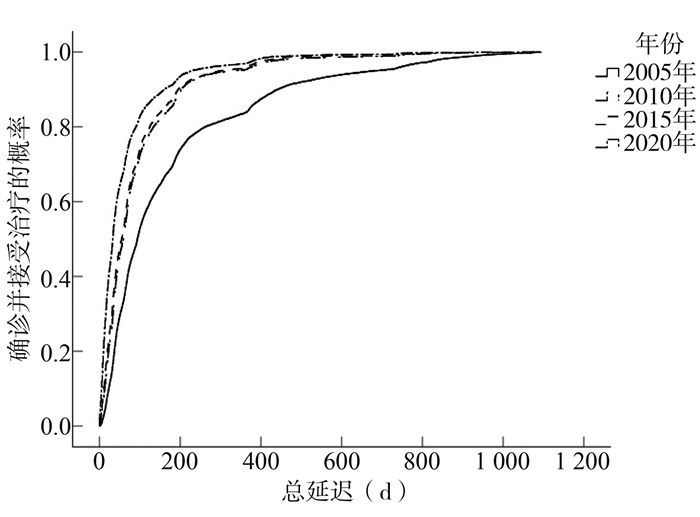
目的 分析“十一五”“十二五”和“十三五”中国结核病防治规划期间云南省病原学阳性肺结核患者总延迟时间的变化趋势,获得影响总延迟发生的影响因素,为减少总延迟的发生提供依据。 方法 利用《结核病管理信息系统》中登记报告的云南省2005年、2010年、2015年和2020年病原学阳性肺结核患者的病案资料。描述最终纳入研究患者的人口学特征、延迟特征。构成比的时间趋势检验用χ2趋势检验,采用Kaplan-Meier法进行组间患者总延迟的比较,估计生存概率并绘制生存函数曲线,用Cox比例风险模型进行患者总延迟发生的多因素分析。 结果 云南省病原学阳性肺结核患者的总延迟整体呈下降趋势,且下降趋势与就诊延迟相似。总延迟中位数由2005年的94 d降至2020年的33 d,2020年患者确诊并接受治疗的概率较2005年增长了2.359倍,不同特征患者的总延迟天数均呈下降趋势。多因素回归分析结果显示,除年份外,女性、高年龄、农民、少数民族、流动人口和复治患者也是发生总延迟的危险因素。 结论 在云南省结核病防控措施的实行下,病原学阳性肺结核患者总延迟天数下降,有效控制了结核病疫情的发展。应侧重于降低总延迟天数较高的危险人群的就诊延迟, 寻求符合成本-效益的主动筛查方式,进一步控制结核病疫情发展。 Abstract:Objective To analyze the trend of total delay of tuberculosis patients with positive etiology in Yunnan Province during the 11th five-year Plan, 12th five-year Plan and 13th five-year Plan for tuberculosis prevention and control, and to obtain the influencing factors of total delay, so as to provide the basis for reducing the occurrence of total delay. Methods Via the tuberculosis management information system(TMIS), we collected medical records of patients with pathogen-positive pulmonary tuberculosis registered in Yunnan Province in 2005, 2010, 2015 and 2020. The demographic characteristics and delay characteristics of the study participants were described. χ2 trend test was used for the time trend test of rate and composition ratio, and the Kaplan-Meier method was used to compare the total delay between groups, and the survival probability was estimated and drawn as a survival function curve. Cox proportional hazard model was used for multivariate analysis of total delay. Results The total delay of positive etiology pulmonary tuberculosis patients in Yunnan Province has declined, and the declining trend was similar to patient delay. The median total delay was reduced from 94 days in 2005 to 33 days in 2020. The probability of patients with pathogenic positive pulmonary tuberculosis being found and receiving treatment in 2020 increased by 2.359 times compared with 2005, and the total delay days of patients with different characteristics showed a downward trend. Multivariate regression analysis showed that besides years, women, older age, farmers, ethnic minorities, floating population and retreatment patients were also risk factors for the total delay. Conclusions With the implementation of tuberculosis prevention, and control measures in Yunnan Province, the total delay days of patients with positive pathogenic tuberculosis decreased significantly, which effectively controlled the development of tuberculosis epidemic. To further control the development of the tuberculosis epidemic, we should pay attention to the risk groups with long total delay days, and seek cost-effective active screening methods to reduce the patient delay of dangerous people. -
Key words:
- Pulmonary tuberculosis /
- Positive etiology /
- Total delay /
- Trend analysis /
- Yunnan Province
-

图 1 2005-2020年病原学阳性肺结核患者总延迟趋势
Figure 1. The total delay trend of pathogenic positive pulmonary tuberculosis patients from 2005 to 2020
表 1 病原学阳性患者的基本情况[n(%)]
Table 1. Characteristics of tuberculosis patients with positive etiology [n(%)]
变量 合计 2005年 2010年 2015年 2020年 χ趋势2值 P值 N=41 106 n=11 500 n=13 251 n=5 200 n=11 155 性别 34.58 <0.001 男 28 327(68.91) 7 684(66.82) 9 202(69.44) 3 660(70.38) 7 781(69.75) 女 12 779(31.09) 3 816(33.18) 4 049(30.56) 1 540(29.62) 3 374(30.25) 年龄(岁) 1 411.49 <0.001 0~ < 15 268(0.65) 94(0.82) 62(0.47) 31(0.60) 81(0.73) 15~ < 25 6 471(15.74) 2 161(18.79) 2 254(17.01) 709(13.63) 1 347(12.08) 25~ < 35 7 750(18.85) 2 644(22.99) 2 736(20.65) 887(17.06) 1 483(13.29) 35~ < 45 7 609(18.51) 2 239(19.46) 2 616(19.74) 1 053(20.25) 1 701(15.25) 45~ < 55 7 192(17.50) 1 735(15.09) 2 146(16.20) 1 015(19.52) 2 296(20.58) 55~ < 65 6 022(14.65) 1 465(12.74) 1 918(14.47) 776(14.92) 1 863(16.70) ≥65 5 794(14.10) 1 162(10.10) 1 519(11.46) 729(14.02) 2 384(21.37) 民族 6 580.92 <0.001 汉族 28 421(69.14) 11 340(98.61) 7 987(60.27) 2 815(54.13) 6 279(56.29) 其他民族 12 685(30.86) 160(1.39) 5 264(39.73) 2 385(45.87) 4 876(43.71) 职业 122.99 <0.001 农民 34 171(83.13) 9 390(81.65) 10 913(82.36) 4 369(84.02) 9 499(85.15) 学生 1 673(4.07) 549(4.77) 470(3.55) 158(3.04) 496(4.45) 其他 5 262(12.80) 1 560(13.57) 1 866(14.08) 673(12.94) 1 160(10.40) 户籍 1 032.58 <0.001 本地 37 644(91.58) 11 056(96.14) 12 481(94.19) 4 520(86.92) 9 587(85.94) 流动 3 462(8.42) 444(3.86) 770(5.81) 680(13.08) 1 568(14.06) 治疗分类 220.60 <0.001 初治 36 594(89.02) 9 879(85.90) 12 155(91.72) 4 678(89.96) 9 882(88.59) 复治 4 512(10.98) 1 621(14.10) 1 096(8.27) 522(10.04) 1 273(11.41)  下载: 导出CSV
下载: 导出CSV
表 2 2005-2020年云南省病原学阳性肺结核患者延迟趋势
Table 2. Delayed trend of pathogenic positive pulmonary tuberculosis patients in Yunnan Province from 2005 to 2020
变量 2005年 2010年 2015年 2020年 总延迟 极值(Min, Max) (0, 1 094) (0, 1 087) (0, 1 095) (0, 1 086) 中位数[M(P25, P75)] 94(43, 207) 59(29, 109) 55(25, 102) 33(13, 72) aHR(95% CI)值 1 1.562(1.521, 1.605) a 1.707(1.648, 1.768) a 2.359(2.291, 2.429) a 就诊延迟 极值(Min, Max) (0, 1 093) (0, 1 084) (0, 1 090) (0, 1 086) 中位数[M(P25, P75)] 59(22, 141) 45(18, 98) 43(16, 92) 26(7, 62) aHR(95% CI)值 1 1.218(1.188, 1.249) a 1.280(1.238, 1.322) a 1.756(1.710, 1.803) a 确诊延迟 极值(Min, Max) (0, 1 087) (0, 821) (0, 731) (0, 1 033) 中位数[M(P25, P75)] 2(1, 24) 2(0, 6) 1(0, 7) 1(0, 7) aHR(95% CI)值 1 1.484(1.443, 1.526) a 1.621(1.564, 1.681) a 1.707(1.656, 1.759) a 治疗延迟 极值(Min, Max) (0, 730) (0, 366) (0, 563) (0, 264) 中位数[M(P25, P75)] 1(0, 2) 1(0, 1) 0(0, 1) 0(0, 0) aHR(95% CI)值 1 1.348(1.312, 1.385) a 1.905(1.838, 1.974) a 2.048(1.989, 2.109) a 注:aCox比例风险回归模型P<0.001。
下载: 导出CSV
表 3 不同特征患者的总延迟趋势
Table 3. Total delay trend of different patient characteristics
变量 2005年 2010年 2015年 2020年 总延迟天数
M(P25, P75)HR(95% CI)值 总延迟天数
M(P25, P75)HR(95% CI)值 总延迟天数
M(P25, P75)HR(95% CI)值 总延迟天数
M(P25, P75)HR(95% CI)值 性别 男 93
(42, 205.75)1 58
(28, 107)1.612
(1.564, 1.663) a53
(24, 100)1.742
(1.674, 1.813) a32
(12, 73)2.278
(2.206, 2.353) a女 96.5
(45, 211)1 61
(31, 114)1.630
(1.559, 1.706) a60
(28, 112.75)1.650
(1.554, 1.751) a34
(13, 72)2.429
(2.316, 2.547) a年龄(岁) 0~ < 15 75
(36, 148.5)1 47
(21.75, 87.75)1.622
(1.167, 2.255) a44
(17, 87)1.895
(1.247, 2.880) a35
(10.5, 66)2.338
(1.712, 3.193) a15~ < 25 74
(37, 176)1 57
(27, 100)1.459
(1.374, 1.549) a48
(22, 91.5)1.600
(1.469, 1.743) a31
(11, 68)2.146
(2.003, 2.299) a25~ < 35 94
(42, 212.75)1 58
(28, 107)1.735
(1.643, 1.834) a56
(25, 108)1.742
(1.613, 1.881) a31
(11, 67)2.599
(2.435, 2.774) a35~ < 45 100
(45, 217)1 62
(30, 114)1.660
(1.568, 1.759) a60
(29, 111)1.694
(1.573, 1.825) a35
(13, 77.5)2.343
(2.197, 2.500) a45~ < 55 104
(47, 242)1 60
(31, 109.25)1.729
(1.621, 1.844) a56
(25, 103)1.885
(1.742, 2.040) a34
(13, 77)2.411
(2.262, 2.571) a55~ < 65 102
(49, 212.5)1 61
(29, 116)1.644
(1.534, 1.761) a58
(27, 104)1.810
(1.657, 1.977) a34
(14, 72)2.403
(2.240, 2.578) a≥65 91
(43, 208)1 59
(27, 112)1.529
(1.416, 1.652) a50
(24.5, 98)1.694
(1.543, 1.860) a32
(13, 71)2.251
(2.096, 2.418) a民族 汉族 94
(43, 207)1 57
(28, 106)1.663
(1.615, 1.712) a53
(25, 97)1.802
(1.729, 1.879) a32
(12, 72)2.419
(2.344, 2.497) a其他民族 94.5
(41.25, 213.5)1 62
(30, 113)1.509
(1.289, 1.766) a57
(25, 112)1.569
(1.337, 1.841) a34
(13, 72)2.133
(1.822, 2.497) a职业 农民 98
(45, 216)1 61
(30, 111)1.649
(1.604, 1.696) a57
(26,104)1.746
(1.684, 1.811) a33
(13, 73)2.382
(2.313, 2.452) a学生 65
(31, 119.5)1 45
(22, 86.5)1.342
(1.185, 1.519) a35
(17, 81.25)1.621
(1.356, 1.938) a29
(10, 65.75)1.965
(1.735, 2.225) a其他 77
(38, 182)1 51
(23, 101)1.554
(1.451, 1.663) a47
(23, 101.5)1.636
(1.493, 1.792) a34
(12, 72)2.141
(1.981, 2.314) a户籍 本地 94
(43, 208)1 59
(29, 108)1.628
(1.586, 1.671) a56
(26, 101)1.725
(1.665, 1.786) a32
(12, 71)2.348
(2.283, 2.414) a流动 96.5
(46.5, 195)1 58
(28, 123)1.469
(1.306, 1.653) a52
(22, 112.5)1.614
(1.430, 1.822) a40
(16, 79)2.138
(1.920, 2.382) a治疗分类 初治 80
(39, 174)1 60
(29, 107)1.394
(1.357, 1.431) a54
(25, 100)1.491
(1.440, 1.544) a32
(13, 70)2.093
(2.035, 2.153) a复治 356
(147, 566.5)1 56
(33, 143.75)3.490
(3.214, 3.790) a64.5
(29, 128.75)3.523
(3.177, 3.906) a41
(14, 125.5)3.917
(3.620, 4.238) a注:aCox比例风险回归模型P<0.001。
下载: 导出CSV
表 4 不同特征患者的总延迟多因素分析
Table 4. The results of total delay of different patient characteristics by Cox regression analysis
变量 β值 sx值 χ2值 HR调整(95% CI) P值 年份(年) 2005 1.000 2010 0.446 0.014 1 038.781 1.562(1.521, 1.605) <0.001 2015 0.535 0.018 890.356 1.707(1.648, 1.768) <0.001 2020 0.858 0.015 3 312.773 2.359(2.291, 2.429) <0.001 性别 男 0.052 0.011 23.525 1.054(1.032, 1.076) <0.001 女 1.000 年龄(岁) <0.001 0~ < 15 0.096 0.068 2.018 1.101(0.964, 1.257) 0.155 15~ < 25 0.095 0.020 23.709 1.100(1.058, 1.142) <0.001 25~ < 35 0.041 0.018 5.327 1.04(1.006, 1.078) 0.021 35~ < 45 -0.009 0.018 0.282 0.991(0.957, 1.026) 0.596 45~ < 55 -0.018 0.018 1.081 0.98(0.948, 1.016) 0.298 55~ < 65 -0.011 0.018 0.325 0.990(0.954, 1.026) 0.569 ≥65 1.000 民族 汉族 0.054 0.012 20.983 1.055(1.031, 1.080) <0.001 其他民族 1.000 职业 <0.001 农民 1.000 学生 0.173 0.030 33.730 1.189(1.121, 1.260) <0.001 其他 0.098 0.016 38.866 1.10(1.069, 1.137) <0.001 户籍 本地 0.117 0.019 38.346 1.124(1.083, 1.167) <0.001 流动 1.000 治疗分类 初治 0.472 0.016 845.229 1.603(1.552, 1.654) <0.001 复治 1.000
下载: 导出CSV
-
[1] 王微. 基于结核病的流行趋势与防控[J]. 世界最新医学信息文摘, 2019, 19(70): 215-238. DOI: 10.19613/j.cnki.1671-3141.2019.70.171.Wang W. Epidemic trend and prevention and control of tuberculosis based on tuberculosis [J]. World Latest Medicine Information, 2019, 19(70): 215-238. DOI: 10.19613/j.cnki.1671-3141.2019.70.171. [2] 姜世闻. 采取综合措施提高肺结核患者病原学检出率[J]. 中国防痨杂志, 2019, 41(5): 477-479. DOI: 10.3969/j.issn.1000-6621.2019.05.001.Jiang SW. Take comprehensive measures to improve the pathogenic detection rate of pulmonary tuberculosis patients [J]. Chin J of Antituberculosis, 2019, 41(5): 477-479. DOI: 10.3969/j.issn.1000-6621.2019.05.001. [3] Chen H, Wang T, Liu L, et al. Trend in risk of delay in diagnosis of new pulmonary tuberculosis in northwest China from 2008 to 2017[J]. BMC Infect Dis, 2019, 19(1): 100. DOI: 10.1186/s12879-019-3725-9. [4] Asefa A, Teshome W. Total delay in treatment among smear positive pulmonary tuberculosis patients in five primary health centers, southern Ethiopia: a cross sectional study [J]. PLoS One, 2014, 9(7): e102884. DOI: 10.1371/journal.pone.0102884. [5] 黄飞, 杜昕, 陈伟, 等. 中国结核病信息管理系统介绍[J]. 中国数字医学, 2011, 6(10): 97-100. DOI: 10.3969/j.issn.1673-7571.2011.10.031.Huang F, Du X, Chen W, et al. Introduction of tuberculosis information management system in China [J]. China Digital Medicine, 2011, 6(10): 97-100. DOI: 10.3969/j.issn.1673-7571.2011.10.031. [6] Yazdani CJ, Rezai MS, Fendereski A, et al. Treatment delay and total delay among pulmonary tuberculosis patients in the north of Iran: application survival data analysis [J]. Tanaffos, 2017, 16(1): 13-21. [7] 方雪晖, 邹铮, 汤莉. 2008-2016年安徽省学生肺结核变化趋势及特征分析[J]. 中华疾病控制杂志, 2017, 21(10): 1039-1043. DOI: 10.16462/j.cnki.zhjbkz.2017.10.017.Fang XH, Zou Z, Tang L. Trend and characteristics of pulmonary tuberculosis in students of Anhui province, 2008-2016[J]. Chin J Dis Control Prev, 2017, 21(10): 1039-1043. DOI: 10.16462/j.cnki.zhjbkz.2017.10.017. [8] Stjepanović M, Škodrić-Trifunović V, Radisavljević -Pavlović S, et al. Patient, healthcare system and total delay in tuberculosis diagnosis and treatment among Serbian population [J]. Acta Clin Croat. 2018, 57(2): 257-263. DOI: 10.20471/acc.2018.57.02.05. [9] Belkina TV, Khojiev DS, Tillyashaykhov MN, et al. Delay in the diagnosis and treatment of pulmonary tuberculosis in Uzbekistan: a cross-sectional study [J]. BMC Infect Dis, 2014, 14(25): 624. DOI: 10.1186/s12879-014-0624-y. [10] 毛宁, 钟威, 梁爽, 等. 辽宁省2017年肺结核患者就诊延迟相关因素分析[J]. 中国热带医学, 2020, 20(1): 61-64. DOI: 10.13604/j.cnki.46-1064/r.2020.01.14.Mao N, Zhong W, Liang S, et al. Relative factors of delay in treatment of pulmonary tuberculosis patients in Liaoning, 2017[J]. China Tropical Medicine, 2020, 20(1): 61-64. DOI: 10.13604/j.cnki.46-1064/r.2020.01.14. [11] 赵燕, 张天华, 柳巍, 等. 陕西省2015年肺结核患者就诊延迟及其相关因素分析[J]. 中国热带医学, 2017, 17(3): 289-292. DOI: 10.13604/j.cnki.46-1064/r.2017.03.19.Zhao Y, Zhang TH, Liu W, et al. Investigation on health seeking delay and relevant factors among pulmonary tuberculosis patients in Shanxi [J]. China Tropical Medicine, 2017, 17(3): 289-292. DOI: 10.13604/j.cnki.46-1064/r.2017.03.19. [12] 李永文. 山东省全球基金项目县户籍与流动人口肺结核患者就诊延迟现状及影响因素研究[D]. 济南: 山东大学, 2011.Li YW. Current situation and factors affecting health seeking delay in tuberculosis in residents and floating population in sample counties of global fund project, Shandong Province [D]. Jinan: Shandong University, 2011. [13] 唐南, 许琳. 云南省2005年与2013年涂阳肺结核患者就诊延迟变化分析[J]. 公共卫生与预防医学, 2015, 26(2): 4. https://www.cnki.com.cn/Article/CJFDTOTAL-FBYF201502006.htmTang N, Xu L. Comparison of the patients with delayed treatment among smear positive TB patients in Yunnan Province between 2005 and 2013[J]. J of Pub Health and Prev Med, 2015, 26(2): 4. https://www.cnki.com.cn/Article/CJFDTOTAL-FBYF201502006.htm [14] Scott LE, Mccarthy K, Gous N, et al. Comparison of Xpert MTB/RIF with other nucleic acid technologies for diagnosing pulmonary tuberculosis in a high HIV prevalence setting: a prospective study [J]. PLoS Medicine, 2011, 8(7): e1001061. DOI: 10.1371/journal.pmed.1001061. [15] Huong NT, Vree M, Duong BD, et al. Delays in the diagnosis and treatment of tuberculosis patients in Vietnam: a cross-sectional study [J]. BMC Public Health, 2007, 13(7): 110. DOI: 10.1186/1471-2458-7-110. [16] Takarinda KC, Harries AD, Nyathi B, et al. Tuberculosis treatment delays and associated factors within the Zimbabwe national tuberculosis program [J]. BMC Public Health, 2015, 15(1): 29. DOI: 10.1186/s12889-015-1437-7. [17] 傅丽娟, 汪业胜, 朱文龙, 等. 湖州市2008-2018年肺结核患者就诊延迟情况及影响因素[J]. 中华疾病控制杂志, 2021, 25(2): 235-239. DOI: 10.16462/j.cnki.Zhjbkz.2021.02.022.Fu LJ, Wang YS, Zhu WL, et al. Consultation delay and influencing factors among pulmonary tuberculosis patients in Huzhou City from 2008 to 2018[J]. Chin J Dis Control Prev, 2021, 25(2): 235-239. DOI: 10.16462/j.cnki.Zhjbkz.2021.02.022. [18] 赵颖, 罗兴能, 李廷荣, 等. 重庆市沙坪坝区肺结核病患者确诊延迟的病例对照研究[J]. 中国社会医学杂志, 2014, 31(1): 61-63. DOI: 10.3969/j.issn.1673-5625.2014.01.023.Zhao Y, Luo XN, Li TR, et al. A case-control study on diagnostic delay of PTB patients in Shapingba district of Chongqing [J]. Chinese Journal of Social Medicine, 2014, 31(1): 61-63. DOI: 10.3969/j.issn.1673-5625.2014.01.023. [19] Bele S, Jiang W, Lu H, et al. Population aging and migrant workers: bottlenecks in tuberculosis control in rural China [J]. PLoS One. 2014, 9(2): e88290. DOI: 10.1371/journal.pone.0088290. [20] 周玉兰, 邓亚利, 冉建朝, 等. 2008-2017年新疆生产建设兵团肺结核患者就诊、确诊延迟及影响因素分析[J]. 现代预防医学, 2018, 45(16): 3014-3018. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYF201816032.htmZhou YL, Deng YL, Ran JC, et al. Analysis of treatment delay, diagnosis delay and influencing factors of tuberculosis patients in Xinjiang production and construction corps from 2008 to 2017[J]. Modern Prevent Med, 2018, 45(16): 3014-3018. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYF201816032.htm [21] Khan MS, Ning Y, Jinou C, et al. Are global tuberculosis control targets overlooking an essential indicator? Prolonged delays to diagnosis despite high case detection rates in Yunnan, China [J]. Health Policy Plan. 2017, 32(2): 15-21. DOI: 10.1093/heapol/czx046. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 275
- HTML全文浏览量: 150
- PDF下载量: 57
- 被引次数: 0