

First-year mortality after antiretroviral therapy initiation among people living with HIV/AIDS in Guangdong from 2016 to 2018
-
摘要:
目的 了解广东省2016-2018年新接受抗逆转录病毒治疗(antiretroviral therapy, ART)的感染者/艾滋病患者(简称HIV/AIDS患者)治疗首年死亡率变化趋势, 比较与探索"广东艾滋病社区综合防治研究项目"广州市示范区、广州市非示范区及广东省其他市的HIV/AIDS患者死亡率差异及原因, 为AIDS死亡防控工作提供依据。 方法 基于国家艾滋病抗病毒治疗信息系统与《中国死因监测数据集》, 分析2016-2018年在广州市第八人民医院新接受ART的HIV/AIDS患者, 治疗首年死亡率和标准化死亡率比(standardized mortality ratio, SMR); 采用Cochran-Armitage趋势检验分析2016-2018年各年新接受治疗患者的治疗相关指标的变化趋势; 采用Cox回归探索不同地区HIV/AIDS患者治疗首年死亡率差异的原因。 结果 2016-2018年共6 447名HIV/AIDS患者新接受ART, 广州市示范区、广州市非示范区和广东省其他市的患者分别为976、3 921和1 550人; 期间死亡152人。2016-2018年广州市示范区患者的治疗首年死亡率下降79.7%, 广州市非示范区患者死亡率下降趋势不明显, 广东省其他市患者死亡率上升18.8%;经标化后, 三组现住址患者的SMR均呈现下降趋势。三组患者的早治疗率随开始治疗年份增加而增加, 但是仅广州市的患者疗效随年份增加改善显著。Cox回归结果显示在校正不同地区患者的基线特征以及项目实施过程中控制效果良好的因素后, 三组现住址患者死亡率差异均无统计学意义(均有P>0.05)。 结论 项目实施下, 广州市HIV/AIDS患者治疗首年死亡率得到控制, 特别是示范区患者首年死亡率在2018年下降至较低水平, 但广东省其他市患者死亡率相对较高且可用较差的基线特征与治疗相关指标解释。对于在广州市接受治疗且居住在广东省其他市的HIV/AIDS患者, 掌握疗效较差原因, 积极促进早治疗以提高ART疗效是降低这部分患者首年死亡率的关键。 Abstract:Objective To estimate the trends in first-year mortality among HIV/AIDS patients newly receiving antiretroviral therapy (ART) in Guangdong Province from 2016 to 2018. To compare the differences in mortality among HIV/AIDS patients from different regions in Guangdong during the"Guangdong AIDS Community Integrated Prevention and Treatment Research Project". Methods We estimated the annual first-year mortality after ART and standardized mortality ratio (SMR) of HIV/AIDS patients receiving ART at Guangzhou Eighth People's Hospital. And we analyzed the changes in patients'treatment characteristics using Cochran-Armitage tests. Finally, we explored the differences in first-year mortality of HIV/AIDS patients from different regions using Cox regressions. Results During 2016-2018, a total of 6 447 HIV/AIDS patients newly started ART. The number of patients in Guangzhou demonstration districts, other districts in Guangzhou and other cities in Guangdong Province were 976, 3 921, and 1 550, among that 152 people died. From 2016 to 2018, first-year mortality in Guangzhou demonstration districts decreased by 79.7%. The mortality in other districts in Guangzhou did not decline significantly, and the mortality of patients in other Cities in Guangdong increased by 18.8%. After standardization, SMR of three groups of patients all decreased.Among three groups, the early-diagnosis rates increased by year. But only HIV/AIDS patients living in Guangzhou had significant improvement in treatment outcome over the year. Cox regressions showed that after adjusting for baseline characteristics and factors being well controlled during the program implementation, differences in mortality rates no longer existed among patients in the three residence groups. Conclusions The first-year mortality of HIV/AIDS patients receiving ART in Guangzhou was well-controlled, especially patients from demonstration districts. But patients in other cities in Guangdong had high mortality, which could be explained by their poor physical conditions. For patients with HIV/AIDS receiving ART in Guangzhou but living in other cities in Guangdong Province, to focus on the poor ART outcomes and actively promote early treatment are crucial in reducing their first-year mortality. -
Key words:
- AIDS /
- Antiretroviral therapy /
- Mortality /
- Temporal trends
-

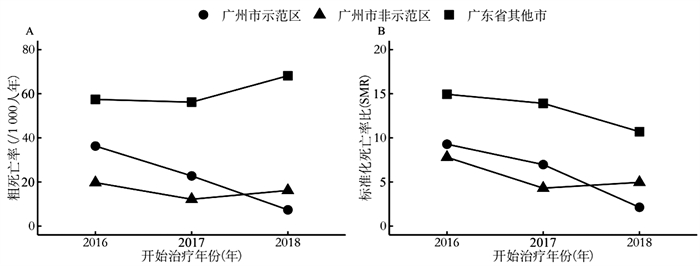
图 1 2016—2018年广东省地区间HIV抗病毒治疗者粗死亡率与标化死亡率比
注:A表示2016—2018年广东省地区间HIV抗病毒治疗者粗死亡率;B表示2016—2018年广东省地区间HIV抗病毒治疗者标准化死亡率比。
Figure 1. Crude mortality and SMR of HIV/AIDS patients receiving ART from different districts in Guangdong Province from 2016 to 2018
表 1 2016—2018年广东省各地区HIV治疗者的基本情况描述[n(%)]
Table 1. Baseline characteristics of HIV/AIDS patients receiving ART from different districts in Guangdong Province during 2016-2018 [n(%)]
变量 合计 现住址 χ2值 P值 广州示范区 广州非示范区 广东省其他市 死亡人数(%) 152(2.4) 19(1.9) 55(1.4) 78(5.0) 开始治疗年份(年) 10.344 0.035 2016 2 215(34.4) 316(32.4) 1 328(33.9) 571(36.8) 2017 2 199(34.1) 352(36.1) 1 316(33.6) 531(34.3) 2018 2 033(31.5) 308(31.6) 1 277(32.6) 448(28.9) 年龄(岁) 130.525 < 0.001 15~<30 2 519(39.1) 366(37.5) 1 654(42.2) 499(32.2) 30~<45 2 298(35.6) 332(34.0) 1 452(37.0) 514(33.2) 45~<60 1 216(18.9) 218(22.3) 6 15(15.7) 383(24.7) ≥60 414(6.4) 60(6.1) 200(5.1) 154(9.9) 性别(男性) 5 613(87.1) 850(87.1) 3 511(89.5) 1 252(81.8) 75.849 < 0.001 感染途径 308.815 < 0.001 同性性行为 3 624(56.2) 564(57.8) 2 458(62.7) 602(38.8) 异性性行为 2 184(33.9) 278(28.5) 1 157(29.5) 749(48.3) 静脉吸毒 168(2.6) 51(5.2) 83(2.1) 34(2.2) 其他 471(7.3) 83(8.5) 223(5.7) 165(10.6) CD4+T淋巴细胞(个/μl) 414.151 < 0.001 ≤50 1 065(16.5) 127(13.0) 434(11.1) 504(32.5) 51~≤200 1 577(24.5) 245(25.1) 951(24.3) 381(24.6) 201~≤350 2 219(34.4) 331(33.9) 1 509(38.5) 379(24.5) >350 1 586(24.6) 273(28.0) 1 027(26.2) 286(18.5) 确诊到治疗间隔(月) 29.238 < 0.001 < 1 3 914(60.7) 566(58.0) 2 403(61.3) 945(61.0) 1~<3 1 090(16.9) 159(16.3) 639(16.3) 292(18.8) 3~<12 504(7.9) 63(6.5) 331(8.5) 110(7.1) ≥12 939(14.6) 188(19.3) 548(14.0) 203(13.1) 基线结核感染情况 113.689 < 0.001 感染 263(4.1) 37(3.8) 95(2.4) 131(8.5) 未感染 6 134(95.1) 928(95.1) 3 806(97.1) 1 400(90.3) 不详 50(0.8) 11(1.1) 20(0.5) 19(1.2) 合计 6 447 976(15.1) 3 921(60.8) 1 550(24.0)  下载: 导出CSV
下载: 导出CSV
表 2 2016—2018年广东省各地区治疗者的治疗期间相关指标趋势性分析[n(%)]
Table 2. Trends of indicators during ART among HIV/AIDS patients from different districts in Guangdong Province from 2016 to 2018[n(%)]
地区 开始治疗年份 |Z|值 P值 2016 2017 2018 广州示范区 确诊后1月内治疗率 157(49.6) 195(55.3) 224(72.7) 5.838 < 0.001 基线CD4+T淋巴细胞≥200个/μl比例 212(67.1) 202(57.4) 190(61.7) 1.405 0.160 未漏服率 226(71.5) 230(65.3) 235(76.2) 1.291 0.197 病毒抑制率 142(44.9) 175(45.7) 169(54.8) 2.481 0.013 增加30% CD4+T淋巴细胞比例 263(83.2) 307(87.2) 274(89.0) 2.098 0.036 广州其他区 确诊后1个月内治疗率 727(54.7) 830(63.0) 879(68.8) 7.420 < 0.001 基线CD4+T淋巴细胞≥200个/μl比例 855(64.4) 849(64.5) 832(65.2) 0.409 0.682 未漏服率 979(73.7) 949(72.1) 935(73.2) 0.298 0.765 病毒抑制率 608(45.7) 604(45.8) 701(54.8) 4.621 < 0.001 增加30% CD4+T淋巴细胞比例 1 155(87.0) 1 140(86.6) 1 118(87.5) 0.431 0.666 广东省其他市 确诊后1个月内治疗率 326(57.0) 336(63.2) 300(66.9) 3.266 0.001 基线CD4+T淋巴细胞≥200个/μl比例 265(46.4) 220(41.4) 180(40.2) 2.050 0.040 未漏服率 397(69.5) 374(70.4) 312(69.6) 0.065 0.949 病毒抑制率 237(41.5) 229(43.1) 203(45.3) 1.213 0.225 增加30% CD4+T淋巴细胞比例 481(84.2) 453(85.3) 380(84.8) 0.287 0.774
下载: 导出CSV
表 3 2016—2018年广东省各地区患者死亡的单因素与校正Cox回归分析
Table 3. Univariate and adjusted Cox regression among HIV/AIDS patients from different districts in Guangdong Province from 2016 to 2018
现住址 模型1a 模型2b 模型3c HRu (95% CI)值 P值 HRa1 (95% CI)值 P值 HRa2 (95% CI)值 P值 广州市示范区 1.00 1.00 1.00 广州市非示范区 0.72 (0.43~1.22) 0.219 0.89 (0.53~1.51) 0.670 0.97 (0.56~1.67) 0.912 广东省其他市 2.67 (1.61~4.40) < 0.001 2.02 (1.21~3.36) 0.007 1.44 (0.84~2.47) 0.178 BIC值 2 596.07 2 483.50 2 003.57 注:a表示现住址与死亡的单因素Cox回归;b表示基于模型1进一步纳入基线年龄、性别、感染途径、基线结核感染情况进行校正;c表示基于模型2进一步纳入基线CD4+T淋巴细胞计数、确诊与治疗时间间隔、治疗后病毒抑制情况以及治疗后CD4+T淋巴细胞增长情况进行校正。
下载: 导出CSV
-
[1] 中华人民共和国国家卫生健康委员会. 2020年全国法定传染病疫情概况[EB/OL]. (2021-03-12) [2021-12-01]. http://www.nhc.gov.cn/jkj/s3578/202103/f1a448b7df7d4760976fea6d55834966.shtml.National Health Commission of the People's Republic of China. Overview of the National Epidemic of Notifiable Infectious Diseases in 2020 [EB/OL]. (2021-03-12) [2021-12-01]. http://www.nhc.gov.cn/jkj/s3578/202103/f1a448b7df7d4760976fea6d55834966.shtml. [2] 中华人民共和国国家卫生健康委员会. 国家卫生计生委办公厅关于调整艾滋病免费抗病毒治疗标准的通知[EB/OL]. (2016-06-15) [2021-12-01]. http://www.nhc.gov.cn/yzygj/s3593/201606/0b0fa78e10dc41328e842b1bf9cd433e.shtml.National Health Commission of the People's Republic of China. Notice of the General Office of the National Health Commission on Adjusting the Standard of Free Antiretroviral Treatment for AIDS [EB/OL]. (2016-06-15) [2021-12-01]. http://www.nhc.gov.cn/yzygj/s3593/201606/0b0fa78e10dc41328e842b1bf9cd433e.shtml. [3] Brown AE, Kall MM, Smith RD, et al. Auditing national HIV guidelines and policies: The United Kingdom CD4 Surveillance Scheme [J]. Open AIDS J, 2012, 6: 149-155. DOI: 10.2174/1874613601206010149. [4] Munthali T, Michelo C, Mee P, et al. Survival of children living with HIV on art in Zambia: a 13-years retrospective cohort analysis [J]. Front Public Health, 2020, 8: 96. DOI: 10.3389/fpubh.2020.00096. [5] 深圳市卫生健康委员会. 十三五国家科技重大专项广东省艾滋病病毒性肝炎等社区综合防治示范区项目在罗湖区启动[EB/OL]. (2019-03-22) [2021-12-01]. http://wjw.sz.gov.cn/xxgk/gzdt/content/post_3158976.html.Shenzhen Municipal Health Commission. The 13th Five-Year National Science and Technology Major Project Guangdong Province was launched in Luohu District [EB/OL]. (2019-03-22) [2021-12-01]. http://wjw.sz.gov.cn/xxgk/gzdt/content/post_3158976.html. [6] 中国疾病预防控制中心. 全国疾病监测系统死因监测数据集[EB/OL]. (2021-01-11) [2021-12-01]. https://ncncd.chinacdc.cn/xzzq_1/202101/t20210111_223706.htm.Chinese Center for Disease Control and Prevention. Disease Surveillance System Cause of Death Surveillance Dataset in China [EB/OL]. (2021-01-11) [2021-12-01]. https://ncncd.chinacdc.cn/xzzq_1/202101/t20210111_223706.htm. [7] Zhang F, Dou Z, Ma Y, et al. Effect of earlier initiation of antiretroviral treatment and increased treatment coverage on HIV-related mortality in China: a national observational cohort study [J]. Lancet Infect Dis, 2011, 11(7): 516-524. DOI: 10.1016/s1473-3099(11)70097-4. [8] Zhu H, Napravnik S, Eron JJ, et al. Decreasing excess mortality of HIV-infected patients initiating antiretroviral therapy: comparison with mortality in general population in China, 2003-2009 [J]. J Acquir Immune Defic Syndr, 2013, 63(5): e150-157. DOI: 10.1097/qai.0b013e3182948d82. [9] Croxford S, Kitching A, Desai S, et al. Mortality and causes of death in people diagnosed with HIV in the era of highly active antiretroviral therapy compared with the general population: an analysis of a national observational cohort [J]. Lancet Public Health, 2017, 2(1): e35-e46. DOI: 10.1016/s2468-2667(16)30020-2. [10] Liu WD, Tsai WC, Hsu WT, et al. Impact of initiation of combination antiretroviral therapy according to the WHO recommendations on the survival of HIV-positive patients in Taiwan [J]. J Microbiol Immunol Infect, 2020, 53(6): 936-945. DOI: 10.1016/j.jmii.2019.03.008. [11] Bisson GP, Ramchandani R, Miyahara S, et al. Risk factors for early mortality on antiretroviral therapy in advanced HIV-infected adults [J]. AIDS, 2017, 31(16): 2217-2225. DOI: 10.1097/qad.0000000000001606. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 320
- HTML全文浏览量: 184
- PDF下载量: 55
- 被引次数: 0