

Association between dietary diversity and obesity metabolic phenotypes in obese adults in Xi'an
-
摘要:
目的 了解西安市成年肥胖人群的膳食多样化与肥胖代谢表型的关系。 方法 数据来源于西北区域自然人群队列中西安城市队列人群的基线调查,选择具有血样且反映代谢表型指标完整的肥胖人群(BMI≥28 kg/m2)1 069例。根据代谢综合征联合国际多学会联合声明的标准定义肥胖代谢表型。参考膳食多样化得分的评价规则,结合中国居民膳食指南构建膳食多样化指标。运用logistic回归分析模型探讨膳食多样化与肥胖代谢表型关系。 结果 研究对象的膳食多样化存在性别差异,不同肥胖代谢表型者的膳食多样化总分差异有统计学意义。与代谢正常肥胖者相比,代谢异常者膳食多样化得分较低[(4.20±1.88)vs.(4.51±1.97), P=0.010],其畜禽肉、鱼虾、蛋、奶及奶制品的摄入较低。控制混杂因素后,与膳食多样化得分最低的肥胖者相比,得分最高者患代谢异常的风险降低38%(OR=0.62, 95% CI: 0.40~0.96),膳食多样化得分每增加一个单位,肥胖者的代谢异常风险降低10% (OR=0.90, 95%CI: 0.82~0.99),这种关联在女性和强体力活动的肥胖人群中更明显。 结论 膳食多样化增加与成年肥胖人群代谢异常风险减少有关联。采取多样化膳食可能是预防和控制肥胖人群代谢异常的重要营养干预措施。 Abstract:Objective To investigate the association between dietary diversity and metabolic phenotypes of obesity in obese adults in Xi'an. Methods Data were from the baseline survey of Xi'an urban population in the northwest natural population cohort. A total of 1 069 obese participants assessed by BMI≥ 28 kg/m2 with blood samples were selected for analysis. Metabolic phenotypes of obesity were defined based on the metabolic syndrome by Joint Interim Statement criteria. By referring to the evaluation rules of dietary diversity score and the Chinese dietary guidelines the index for dietary diversity was establish. Logistic regression model was used to explore the association between dietary diversity and metabolic phenotypes of obesity. Results There were gender differences in dietary diversity. The total dietary diversity score of obesity participants with different metabolic phenotypes was significantly different. Compared with metabolically healthy obesity, the total dietary diversity score of participants with metabolically unhealthy obesity was lower [(4.20±1.88)vs.(4.51±1.97), P=0.010], mainly reflecting lower intake of meat, poultry, fish, eggs and dairy. After controlling for confounding factors, the participants with the highest score had a 38% lower risk of metabolic abnormalities compared to those with the lowest dietary diversity score (OR=0.62, 95% CI: 0.40-0.96). For each unit increase in dietary diversity score, the risk of metabolic abnormalities in obese people decreased by 10% (OR=0.90, 95% CI: 0.82-0.99), and this association was more obvious in women and strong metabolite equivalents obese people. Conclusions Increased dietary diversity may be associated with reduced risk of metabolic abnormalities in obese adults. Adopting diversified diet may be an important nutritional intervention to prevent and control metabolic abnormalities in obese people. -
Key words:
- Dietary diversity /
- Metabolic disorder /
- Metabolic phenotypes /
- Obesity
-

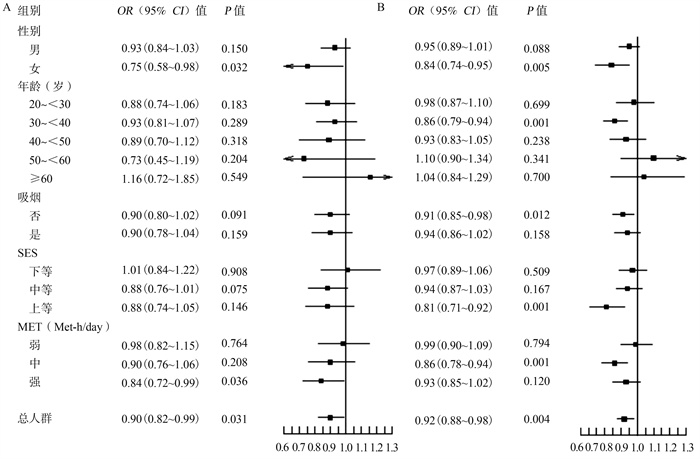
图 1 人群膳食多样化与肥胖代谢表型关联的亚组分析
注:图1A:BMI≥28 kg/m2;图1B:BMI≥25 kg/m2。
Figure 1. Subgroup analysis of the association of dietary diversity and obesity metabolic phenotypes in the population
表 1 研究对象的基本特征(x±s)
Table 1. Basic characteristics of the research object (x±s)
变量 总人群膳食多样化得分 t/χ2值 P值 肥胖代谢表型 t/χ2值 P值 T1(最低)(n=353) T2(n=413) T3(最高)(n=303) MHO(n=417) MUO(n=652) 年龄(岁) 39.1±11.9 40.7±13.3 39.3±12.7 0.28 0.778 38.4±12.3 40.6±12.8 2.89 0.004 男性[n(%)] 298(84.4) 302(73.1) 237(78.2) 14.29 0.001 330(79.1) 507(77.8) 0.28 0.594 BMI(kg/m2) 30.3±2.2 30.3±2.2 30.1±1.9 -1.28 0.200 29.9±1.9 30.4±2.2 3.94 <0.001 吸烟a[n(%)] 167(48.0) 166(40.4) 120(39.7) 5.96 0.051 170(41.0) 283(43.8) 0.84 0.361 体力活动b(Met-h/day) 30.2(25.4, 35.1) 30.5(25.0, 36.8) 33.5(27.9, 40.7) 3.35 0.001 32.1(26.3, 38.2) 30.6(25.3, 36.4) -2.17 0.031 SES 18.4±3.3 18.3±3.3 18.8±3.1 1.47 0.143 18.9±3.1 18.3±3.3 -3.03 0.003 WC(cm) 97.3±7.1 97.5±6.8 97.7±7.7 0.54 0.592 96.6±7.0 98.0±7.3 2.34 0.020 FPG(mmol/L) 5.1±1.2 5.2±1.7 5.1±1.4 -0.08 0.936 4.7±0.5 5.4±1.8 7.40 <0.001 TG(mmol/L) 2.2±1.5 2.1±1.4 2.1±1.4 -1.20 0.231 1.4±0.6 2.6±1.6 14.47 <0.001 HDL-C(mmol/L) 1.1±0.2 1.1±0.2 1.1±0.3 2.31 0.021 1.2±0.2 1.0±0.2 -15.28 <0.001 SBP(mm Hg) 131.4±14.7 130.7±14.8 128.0±14.6 -2.90 0.004 124.4±13.3 133.9±14.5 10.80 <0.001 DBP(mm Hg) 86.2±11.6 85.0±11.8 83.5±11.8 -2.96 0.003 80.0±10.4 88.2±11.6 11.69 <0.001 注:a该指标存在缺失值;b该指标为[M(P25, P75)]。  下载: 导出CSV
下载: 导出CSV
表 2 不同肥胖代谢表型的人群膳食多样化得分情况
Table 2. Dietary diversity scores of people with different obesity metabolic phenotypes
食物类别 MHO(n=417) MUO (n=652) t值 P值 M sx值 M sx值 谷类薯类及杂豆 0.86 0.35 0.85 0.35 0.26 0.795 蔬菜类 0.88 0.33 0.87 0.33 0.29 0.777 水果类 0.68 0.47 0.65 0.48 0.85 0.394 畜禽肉类 0.55 0.50 0.49 0.50 2.09 0.037 鱼虾类 0.10 0.30 0.06 0.24 2.13 0.042 蛋类 0.54 0.50 0.48 0.50 2.05 0.041 奶类及奶制品 0.44 0.50 0.37 0.48 2.31 0.022 大豆类及坚果 0.46 0.50 0.43 0.49 1.17 0.243 膳食多样化总分 4.51 1.97 4.20 1.88 2.58 0.010
下载: 导出CSV
表 3 膳食多样化与肥胖代谢表型之间的关联性分析
Table 3. Correlation analysis between dietary diversity and metabolic phenotypes of obesity
模型 膳食多样化得分[M(P25, P75)] P趋势值 T1 (最低) T2 T3 (最高) MUO/总人数 226/353 264/413 162/303 模型1 a 1.00(参照) 0.97 (0.74, 1.34) 0.65 (0.47, 0.88) 0.007 模型2 b 1.00(参照) 0.98 (0.73, 1.32) 0.64 (0.47, 0.88) 0.006 模型3 c 1.00(参照) 1.19 (0.79, 1.80) 0.60 (0.39, 0.93) 0.022 模型4 d 1.00(参照) 1.21 (0.80, 1.84) 0.62 (0.40, 0.96) 0.025 注:a模型1:未调整模型;b模型2:调整年龄、性别因素;c模型3:调整年龄、性别、吸烟、METs及SES;d模型4:调整年龄、性别、吸烟、METs、SES及BMI。
下载: 导出CSV
-
[1] WHO. World Health Organization 2016[EB/OL]. (2020-03-19)[2021-10-19]. http://www.who.int/mediacentre/factsheets/fs311/en/. [2] 刘月姣. 《中国居民营养与慢性病状况报告(2020年)》发布[J]. 中国食物与营养, 2020, 26(12): 2. DOI: 10.19870/j.cnki.11-3716/ts.2020.12.001.Liu YJ. Report on Chinese residents' chronic diseases and nutrition 2020[J]. Food Nutr China, 2020, 26(12): 2. DOI: 10.19870/j.cnki.11-3716/ts.2020.12.001. [3] Kramer CK, Zinman B, Retnakaran R. Are metabolically healthy overweight and obesity benign conditions?: a systematic review and meta-analysis[J]. Ann Intern Med, 2013, 159(11): 758-769. DOI: 10.7326/0003-4819-159-11-201312030-00008. [4] Gharooi Ahangar O, Javanrouh N, Daneshpour MS, et al. Genetic markers and continuity of healthy metabolic status: tehran cardio-metabolic genetic study (TCGS)[J]. Sci Rep, 2020, 10(1): 13600. DOI: 10.1038/s41598-020-70627-5. [5] Stefan N, Kantartzis K, Machann J, et al. Identification and characterization of metabolically benign obesity in humans[J]. Arch Intern Med, 2008, 168(15): 1609-1616. DOI: 10.1001/archinte.168.15.1609. [6] Hossein F, Mina D, Farshad T, et al. The association of dietary approach to stop hypertension (DASH) diet with metabolic healthy and metabolic unhealthy obesity phenotypes[J]. Sci Rep, 2019, 9(1): 18690. DOI: 10.1038/s41598-019-55285-6. [7] Yanovski SZ, Yanovski JA. Toward precision approaches for the prevention and treatment of obesity[J]. JAMA, 2018, 319(3): 223-224. DOI: 10.1001/jama.2017.20051. [8] Verger EO, Le Port A, Borderon A, et al. Dietary diversity indicators and their associations with dietary adequacy and health outcomes: a systematic scoping review[J]. Adv Nutr, 2021, 12(5): 1659-1672. DOI: 10.1093/advances/nmab009. [9] Milenkovic T, Bozhinovska N, Macut D, et al. Mediterranean diet and type 2 diabetes mellitus: a perpetual inspiration for the scientific world. a review[J]. Nutrients, 2021, 13(4): 1307. DOI: 10.3390/nu13041307. [10] Abdurahman AA, Bule M, Azadbakhat L, et al. The association between diet quality and obesity-related metabolic risks[J]. Hum Antibodies, 2020, 28(1): 1-9. DOI: 10.3233/HAB-190387. [11] Phillips CM, Dillon C, Harrington JM, et al. Defining metabolically healthy obesity: role of dietary and lifestyle factors[J]. PLoS One, 2013, 8(10): e76188. DOI: 10.1371/journal.pone.0076188. [12] Park YM, Steck SE, Fung TT, et al. Mediterranean diet, dietary approaches to stop hypertension (DASH) style diet, and metabolic health in U.S. adults[J]. Clin Nutr, 2017, 36(5): 1301-1309. DOI: 10.1016/j.clnu.2016.08.018. [13] Li C, Liu YZ, Shi GS, et al. Cohort profile: regional ethnic cohort study in northwest China[J]. Int J Epidemiol, 2022, 51(2): e18-e26. DOI: 10.1093/ije/dyab212. [14] 王佳丽, 陈祚, 张林峰, 等. 新疆地区居民代谢健康型肥胖的患病率及影响因素[J]. 心脑血管病防治, 2017, 17(3): 164-168, 178. DOI: 10.3969/j.issn.1009-816x.2017.03.02.Wang JL, Chen Z, Zhang LF, et al. Prevalence and determinants of metabolic health obesity in Xinjiang population[J]. Prevention and Treatment of Cardio-Cerebral-Vascular Disease, 2017, 17(3): 164-168, 178. DOI: 10.3969/j.issn.1009-816x.2017.03.02. [15] Agustina R, Nadiya K, Andini EA, et al. Associations of meal patterning, dietary quality and diversity with anemia and overweight-obesity among Indonesian school-going adolescent girls in West Java[J]. PLoS One, 2020, 15(4): e0231519. DOI: 10.1371/journal.pone.0231519. [16] Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity[J]. Circulation, 2009, 120(16): 1640-1645. DOI: 10.1161/circulationaha.109.192644. [17] Bennett DA, Du H, Clarke R, et al. Association of physical activity with risk of major cardiovascular diseases in Chinese men and women[J]. JAMA Cardiol, 2017, 2(12): 1349-1358. DOI: 10.1001/jamacardio.2017.4069. [18] Low S, Chin MC, Ma S. Who expert consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies[J]. Lancet, 2004, 363(9403): 157-163. DOI: 10.1016/S0140-6736(03)15268-3. [19] Telle-Hansen VH, Christensen JJ, Formo GA, et al. A comprehensive metabolic profiling of the metabolically healthy obesity phenotype[J]. Lipids Health Dis, 2020, 19(1): 90. DOI: 10.1186/s12944-020-01273-z. [20] Ruel MT. Operationalizing dietary diversity: a review of measurement issues and research priorities[J]. J Nutr, 2003, 133(11 Suppl 2): 3911S-3926S. DOI: 10.1093/jn/133.11.3911S. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 433
- HTML全文浏览量: 280
- PDF下载量: 57
- 被引次数: 0