

BMI, WC, and waist-hip ratio and the risk of death in type 2 diabetes mellitus: a cohort study
-
摘要:
目的 了解淮安市2型糖尿病(diabetes mellitus type 2,T2DM)患者不同肥胖指标对其死亡风险的影响。 方法 将淮安市2013年1月1日―2020年12月31日队列随访的9 759例T2DM患者与死因监测平台进行匹配,确定死亡病例。根据BMI、WC、腰臀比(waist-to-hip ratio,WHR)对随访人群进行分组,采用Cox比例风险模型探究肥胖指标对于T2DM患者全死因死亡风险。随后采用敏感性分析,剔除吸烟人群、随访第1年死亡者、基线患心脑血管病者后分析全死因死亡风险情况。 结果 不同年龄、WC、WHR及其他指标的人群BMI差异均有统计学意义(均有P<0.05)。且调整混杂因素后发现,在超重和肥胖人群与正常人群相比死亡风险分别下降17%和27%,差异均有统计学意义(均有P<0.05)。患者WC与非中心性肥胖相比,中心性肥胖前期和中心性肥胖时期均可以降低死亡风险,不同WHR人群死亡风险差异无统计学意义。 结论 目前死亡风险存在“肥胖悖论”现象,研究发现超重和肥胖人群以及中心性肥胖前期死亡风险具有保护作用。 Abstract:Objective To investigate the effects of different obesity indicators on the risk of death in diabetes mellitus type 2 (T2DM) patients in Huai 'an City. Methods A total of 9 759 T2DM patients were followed up in Huai 'an City from 2013 to 2020, and the cause of death was matched through the cause of death monitoring platform. The follow-up population was classified according to BMI, WC, waist-to-hip ratio (WHR), and Cox proportional risk model was adopted to explore the effect of obesity indicators on all-cause mortality risk of T2DM patients. Sensitivity analysis was then used to exclude smokers, those with less than three years of follow-up, and those who died in the first year of follow-up, and baseline patients with cardiovascular and cerebrovascular risk for all-cause mortality. Results The research results indicated the BMI groups in different age, WC, WHR and other indexes were different (P < 0.05). After adjusting for confounding factors, it was found that the risk of death decreased by 17% and 27% in overweight and obese people compared with normal people, respectively, with statistical significance (P < 0.05). Compared with non-central obesity, the waist circumference of patients with central obesity can reduce the risk of death in both pre-central obesity and central obesity, and there was no statistical significance in the risk of death among people with different WHR ratios. Conclusions The "obesity paradox" exists in the risk of death. It is found that BMI has a protective effect on the risk of death in overweight and obesity, as well as in the early stage of central obesity. -
Key words:
- Diabetes type 2 /
- Baby Mass Index /
- Waist circumference /
- Risk of death
-

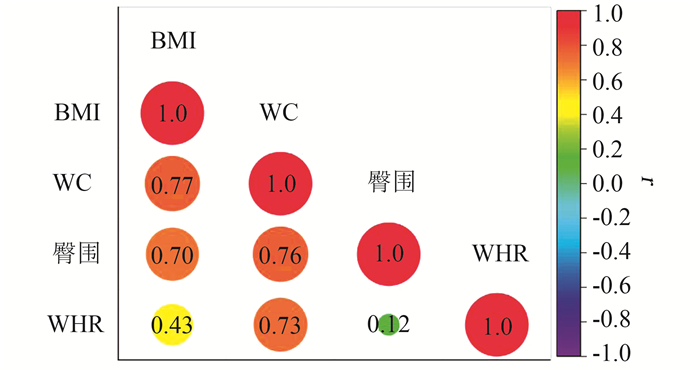
图 1 全人群中肥胖指标之间相关性分析
Figure 1. Correlation analysis of obesity indicators in the whole population

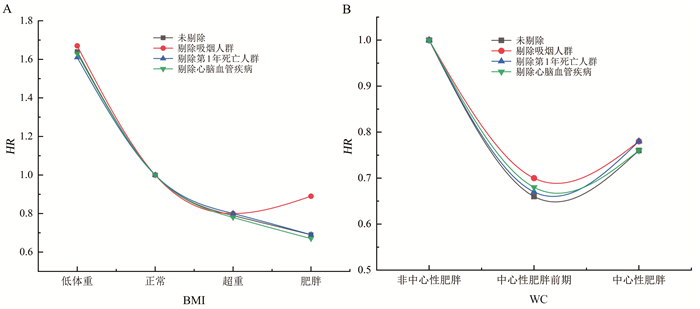
图 2 BMI和WC与全死因死亡风险的敏感性分析
注:采用Cox回归模型调整性别、年龄、文化程度、婚姻状况、家庭年收入、FPG、HbA1C、饮酒、冠心病、糖尿病病程、糖尿病用药、高血压、脑卒中、血脂异常、冠心病等。
Figure 2. Sensitivity analysis of BMI and WC with all-cause mortality risk
表 1 不同BMI和WC人群基线特征[n(%)]
Table 1. Baseline characteristics of participants with different BMI and WC [n(%)]
变量及分类 BMI F/χ2值 P值 腰围分组 F/χ2值 P值 正常 低体重 超重 肥胖 非中心性肥胖 中心性肥胖前期 中心性肥胖 人数(n) 2 804(28.9) 117(1.2) 4 341(44.7) 2 454(25.3) 2 742(28.2) 1 952(20.1) 5 022(51.7) 性别(男) 1 041(37.1) 32(27.4) 1 682(38.7) 917(37.4) 7.83 0.044 1 240(45.2) 725(37.1) 1 707(34.0) 95.61 0.013 年龄(x±s, 岁) 61.93±10.18 63.67±10.16 61.33±10.02 61.41±10.03 3.96 < 0.001 61.22±10.31 60.69±9.95 62.07±9.96 15.33 < 0.001 静态行为时间[M(P75, P25), h/d] 2.5 (1.7, 4.0) 3.0 (2.0, 4.0) 3.0 (2.0, 4.2) 3.0 (2.0, 4.8) 2.27 0.007 2.5 (1.5, 4.0) 3.0 (2.0, 4.0) 3.0 (2.0, 5.0) 8.25 < 0.001 血糖 9.17±4.75 10.01±6.30 8.82±3.96 8.62±3.46 11.15 < 0.001 9.08±4.84 8.98±4.40 8.74±3.56 6.85 0.001 HbA1C 7.87±2.32 8.19±2.89 7.72±1.90 7.78±1.80 4.78 < 0.001 7.78±2.32 7.76±2.02 7.80±1.84 0.28 0.759 吸烟 14.73 0.002 43.85 < 0.001 是 888(31.7) 42(35.9) 1 268(29.2) 669(27.3) 943(34.4) 543(27.8) 1 381(27.5) 饮酒 16.83 0.001 2.61 0.271 是 415(14.8) 14(12.0) 792(18.3) 427(17.4) 489(17.8) 314(16.1) 845(16.8) 文化程度 40.30 < 0.001 2.05 0.359 未接受正规教育 1 208(43.3) 71(60.7) 1 702(39.5) 1 003(41.1) 1 106(40.6) 787(40.6) 2 091(41.9) 小学 789(28.3) 30(25.6) 1 203(27.9) 703(28.8) 843(30.9) 527(27.2) 1 355(27.2) 初中 517(18.5) 14(12.0) 871(20.2) 500(20.5) 525(19.3) 418(21.5) 959(19.2) 高中及以上 276(9.9) 2(1.7) 531(12.3) 232(9.5) 250(9.2) 208(10.7) 583(11.7) 婚姻状况 39.43 < 0.001 18.48 < 0.001 在婚 2 309(82.9) 95(81.9) 3 791(88.0) 2 109(86.7) 2 278(83.7) 1 686(87.0) 4 340(87.1) 家庭年收入(万元) 33.80 < 0.001 44.57 < 0.001 <1 738(26.5) 50(42.7) 1 022(23.7) 563(23.1) 772(28.4) 454(23.4) 1 147(23.0) 1~3 1 035(37.1) 42(35.9) 1 601(37.2) 912(37.4) 1 028(37.8) 741(38.2) 1 821(36.5) 4~10 921(33.0) 22(18.8) 1 508(35.0) 869(35.7) 842(31.0) 671(34.6) 1 807(36.2) >10 93(3.3) 3(2.6) 175(4.1) 93(3.8) 78(2.9) 75(3.9) 211(4.2) 糖尿病病程(年) 5.09 0.165 19.42 < 0.001 < 2 829(29.6) 34(29.1) 1 256(28.9) 748(30.5) 870(31.7) 595(30.5) 1 402(27.9) 2~4 771(27.5) 27(23.1) 1 293(29.8) 729(29.7) 789(28.8) 575(29.5) 1 456(29.0) 5~9 649(23.1) 31(26.5) 1 002(23.1) 549(22.4) 632(23.0) 434(22.2) 1 165(23.2) ≥10 555(19.8) 25(21.4) 790(18.2) 428(17.4) 451(16.4) 348(17.8) 999(19.9) 高血压 356.59 < 0.001 243.87 < 0.001 是 1 685(60.3) 54(46.2) 3 109(71.8) 2 028(82.7) 1 655(60.5) 1 348(69.2) 3 873(77.3) 血脂异常 312.19 < 0.001 324.40 < 0.001 是 1 159(41.3) 25(21.4) 2 422(55.8) 1 545(63.0) 1 078(39.3) 1 028(52.7) 3 045(60.7) 冠心病 49.65 < 0.001 35.42 < 0.001 是 208(7.4) 9(7.7) 436(10.0) 354(14.4) 195(7.1) 164(8.4) 648(12.9) 脑卒中 27.71 < 0.001 10.89 0.004 是 317(11.3) 2(1.7) 570(13.1) 373(15.2) 304(11.1) 245(12.6) 713(14.2)  下载: 导出CSV
下载: 导出CSV
表 2 BMI对死亡风险的Cox回归模型分析
Table 2. Cox regression model of BMI and death risk
BMI 死亡人数(n) 随访人年 死亡密度(‰) 死亡率(%) 模型1 模型2 模型3 HR(95% CI)值 P值 HR(95% CI)值 P值 HR(95% CI)值 P值 正常 448 217 078 2.06 1.59 1.00 1.00 1.00 低体重 32 8 669 3.69 2.74 1.80(1.26~2.58) < 0.001 1.55(1.07~2.23) 0.020 1.61(1.12~2.33) 0.010 超重 532 344 194 1.54 1.23 0.75(0.66~0.85) < 0.001 0.83(0.73~0.94) < 0.001 0.80(0.71~0.91) < 0.001 肥胖 276 196 854 1.40 1.12 0.68(0.58~0.79) < 0.001 0.74(0.64~0.87) < 0.001 0.71(0.60~0.82) < 0.001 注:死亡率为死亡人数/BMI各组人数。模型1为未调整混杂因素前,BMI对于患者死亡风险的风险比;模型2为调整性别、年龄、文化程度、婚姻状况、家庭年收入、静态行为时间、吸烟、饮酒等的风险情况;模型3为在模型2基础上、调整FPG、HbA1C、糖尿病治疗率、糖尿病病程、高血压、脑卒中、血脂异常、冠心病等因素。Pearson相关分析显示BMI与WC相关性较强(r=0.77),故不同时纳入研究中。
下载: 导出CSV
表 3 WC和WHP对死亡风险的Cox回归模型分析
Table 3. Cox regression analysis of WC and the WHP circumference on mortality risk
变量 死亡人数 随访人年 死亡密度(‰) 死亡率(%) 模型1 模型2 模型3 HR(95% CI)值 P值 HR(95% CI)值 P值 HR(95% CI)值 P值 WC分组 非中心性肥胖 438 212 946 1.06 1.60 1.00 1.00 1.00 中心性肥胖前期 200 156 134 1.28 1.02 0.62(0.53~0.73) < 0.001 0.71(0.60~0.84) < 0.001 0.67(0.57~0.80) < 0.001 中心性肥胖 650 397 973 1.63 1.29 0.80(0.70~0.90) < 0.001 0.84(0.74~0.95) 0.010 0.78(0.69~0.89) < 0.001 WHP 非中心性肥胖 459 258 966 1.77 1.39 1.00 1.00 1.00 中心性肥胖 829 508 087 1.63 1.29 0.92(0.82~1.03) 0.150 0.98(0.87~1.11) 0.980 0.93(0.82~1.04) 0.200 注:死亡率:死亡人数/WC(WHP)各组人数。模型调整同表 2。
下载: 导出CSV
-
[1] Hainer V, Aldhoon-Hainerová I. Obesity paradox does exist[J]. Diabetes Care, 2013, 36(Suppl 2): S276-S281. DOI: 10.2337/dcS13-2023. [2] Bouchi R, Asakawa M, Ohara N, et al. Indirect measure of visceral adiposity'A Body Shape Index' (ABSI) is associated with arterial stiffness in patients with type 2 diabetes[J]. BMJ Open Diabetes Res Care, 2016, 4(1): e000188. DOI: 10.1136/bmjdrc-2015-000188. [3] Gu D, He J, Duan X, et al. Body weight and mortality among men and women in China[J]. JAMA, 2006, 295(7): 776-783. DOI: 10.1001/jama.295.7.776. [4] Chung WS, Ho FM, Cheng NC, et al. BMI and all-cause mortality among middle-aged and older adults in Taiwan: a population-based cohort study[J]. Public Health Nutr, 2015, 18(10): 1839-1846. DOI: 10.1017/S136898001400281X. [5] Flegal KM, Graubard BI, Williamson DF, et al. Excess deaths associated with underweight, overweight, and obesity: an evaluation of Potential Bias[J]. Vital Health Stat 3, 2018, (42): 1-21. DOI: 10.1001/jama.298.17.2028. [6] Krakauer NY, Krakauer JC. A new body shape index predicts mortality hazard independently of body mass index[J]. PLoS One, 2012, 7(7): e39504. DOI: 10.1371/journal.pone.0039504. [7] 李嘉琛, 吕筠, 高萌, 等. 中国成年人体质指数和腰围与主要慢性病风险的关联研究[J]. 中华流行病学杂志, 2019, 40(12): 1541-1547. DOI: 10.3760/cma.j.issn.0254-6450.2019.12.007.Li JC, Lyu J, Gao M, et al. Association of body mass index and waist circumference with major chronic diseases in Chinese[J]. Chin J Epidemiol, 2019, 40(12): 1541-1547. DOI: 10.3760/cma.j.issn.0254-6450.2019.21.007. [8] Rexrode KM, Carey VJ, Hennekens CH, et al. On the achievement of comprehensive control targets among type 2 diabetic patients managed by communities in Jiangsu Province[J]. JAMA, 1998, 280(21): 1843-1848. DOI: 10.1001/jama.280.21.1843. [9] 苏健, 覃玉, 沈冲, 等. 江苏省社区管理2型糖尿病患者综合控制情况分析[J]. 中华内分泌代谢杂志, 2018, 34(2): 112-120. DOI: 10.3760/cma.j.issn.1000-6699.2018.02.005.Su J, Qin Y, Shen C, et al. On the achievement of comprehensive control targets among type 2 diabetic patients managed by communities in Jiangsu Province[J]. Chin J Endocrinol Metab, 2018, 34(2): 112-120. DOI: 10.3760/cma.j.issn.1000-6699.2018.02.005. [10] 中国肥胖问题工作组. 中国成人超重与肥胖症预防与控制指南(节录)[J]. 营养学学报, 2004, 26(1): 1-4. DOI: 10.3321/j.issn:0512-7955.2004.01.001.Group of China Obesity Task Force. Guidelines for prevention and control of overweight and obesity in Chinese adults (excerpt)[J]. Acta Nutrimenta Sinca, 2004, 26(1): 1-4. DOI: 10.3321/j.issn:0512-7955.2004.01.001. [11] 周北凡. 三我国成人体质指数和腰围对相关疾病危险因素异常的预测价值―我国成人适宜体质指数和腰围切点的研究[C]//中华医学会. 内分泌腺及全身性疾病-中华医学会第六次全国内分泌学术会议论文汇编. 北京: 中华医学会, 2001: 33.Zhou BF. Three The predictive value of body mass index and waist circumference of Chinese adults on the abnormality of risk factors for related diseases-a study on the cut-off point of suitable body mass index and waist circumference of Chinese adults[C]//Chinese Medical Association. Endocrine glands and systemic diseases-proceedings of the sixth national endocrine academic conference of the Chinese Medical Association. Beijing: Chinese Medical Association, 2001: 33. [12] 李瑞杰. 中国高血压防治指南(2010年修订版)重点内容介绍[J]. 中国临床医生, 2012, 40(2): 69-72. DOI: 10.3969/j.issn.1008-1089.2012.02.027.Li RJ. Introduction of key contents of hypertension prevention and treatment guidelines in China (Revised Edition in 2010)[J]. Chin Clin Dr, 2012, 40(2): 69-72. DOI: 10.3969/j.issn.1008-1089.2012.02.027. [13] 中国高血压防治指南修订委员会, 高血压联盟(中国), 中华医学会心血管病学分会, 等. 中国高血压防治指南(2018年修订版)[J]. 中国心血管杂志, 2019, 24(1): 24-56. DOI: 10.3969/j.issn.1007-5410.2019.01.002.Writing Group of 2018 Chinese Guidelines for the Management of Hypertension, Chinese Hypertension League, Chinese Society of Cardiology, et al. 2018 Chinese guidelines for the management of hypertension[J]. Chin J Cardiovasc Med, 2019, 24(1): 24-56. DOI: 10.3969/j.issn.1007-5410.2019.01.002. [14] So E, Kim J, Joo S, et al. Association of dietary patterns with overweight risk and all-cause mortality in children with cancer[J]. Nutr Res Pract, 2017, 11(6): 492-499. DOI: 10.4162/nrp.2017.11.6.492. [15] Jayedi A, Soltani S, Zargar MS, et al. Central fatness and risk of all cause mortality: systematic review and dose-response meta-analysis of 72 prospective cohort studies[J]. BMJ, 2020, 370: m3324. DOI: 10.1136/bmj.m3324. [16] Zhang C, Rexrode KM, van Dam RM, et al. Abdominal obesity and the risk of all-cause, cardiovascular, and cancer mortality: sixteen years of follow-up in US women[J]. Circulation, 2008, 117(13): 1658-1667. DOI: 10.1161/CIRCULATIONAHA.107.739714. [17] 刘雪娇, 王炳源, 任永成, 等. 高血压人群中体质指数与全死因死亡风险的队列研究[J]. 中华流行病学杂志, 2018, 39(7): 914-919. DOI: 10.3760/cma.j.issn.0254-6450.2018.07.010.Liu XJ, Wang BY, Ren YC, et al. Cohort study on body mass index and risk of all-cause mortality among hypertensive population[J]. Chin J Epidemiol, 2018, 39(7): 914-919. DOI: 10.3760/cma.j.issn.0254-6450.2018.07.010. [18] Tobias DK, Pan A, Jackson CL, et al. Body-mass index and mortality among adults with incident type 2 diabetes[J]. N Engl J Med, 2014, 370(3): 233-244. DOI: 10.1056/NEJMoa1304501. [19] Lee JY, Kim HC, Kim C, et al. Underweight and mortality[J]. Public Health Nutr, 2016, 19(10): 1751-1756. DOI: 10.1017/s136898001500302x. [20] Jackson CL, Yeh HC, Szklo M, et al. Body-mass index and all-cause mortality in US adults with and without diabetes[J]. J Gen Intern Med, 2014, 29(1): 25-33. DOI: 10.1007/s11606-013-2553-7. [21] Antonopoulos AS, Oikonomou EK, Antoniades C, et al. From the BMI paradox to the obesity paradox: the obesity-mortality association in coronary heart disease[J]. Obes Rev, 2016, 17(10): 989-1000. DOI: 10.1111/obr.12440. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 313
- HTML全文浏览量: 130
- PDF下载量: 34
- 被引次数: 0