

The relationship between a plant-based diet and death in the elderly aged 65 and over in China
-
摘要:
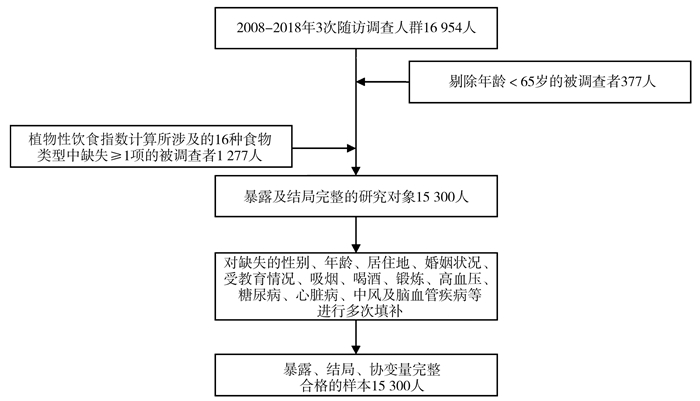
目的 探讨老年人植物性饮食与死亡之间的关系。 方法 基于中国老年健康和家庭幸福调查(Chinese Longitudinal Healthy Longevity and Happy Family Study, CLHLS-HF)数据,分析15 300份样本在2008―2018年随访调查资料。以植物性饮食指数(plant-based diet index, PDI)、不健康的植物性饮食指数(unhealthy plant-based diet index, UPDI)作为评估植物性饮食情况的指标,分别按五分位数分组,分为Q1、Q2、Q3、Q4、Q5共5组。采取Cox回归分析构建模型,研究PDI、UPDI对于65岁及以上老年人死亡的影响。 结果 调整人口学特征、健康行为和基础疾病混杂因素后,PDI与死亡存在统计学关联(P < 0.001),以Q1为对照组,Q3(HR=0.900, 95% CI: 0.832~0.974)、Q4(HR=0.872, 95% CI: 0.804~0.947)、Q5组(HR=0.779, 95% CI: 0.715~0.850)人群死亡风险分别减少10.00%、12.80%、22.10%,Q2组差异无统计学意义;UPDI与死亡存在统计学关联(P < 0.001),相较Q1组,Q3(HR=1.182, 95% CI: 1.080~1.294)、Q4(HR=1.206, 95% CI: 1.101~1.321)、Q5组(HR=1.210, 95% CI: 1.104~1.327)人群死亡风险分别增加18.20%、20.60%、21.00%,Q2组差异无统计学意义。随着PDI分数的上升,人群死亡风险呈下降的趋势;随着UPDI分数的上升,人群死亡风险呈上升的趋势(均P趋势 < 0.001)。 结论 基于CLHLS-HF人群可知,减少植物性食物尤其是健康的植物性食物摄入频率会增加老年人死亡的风险。 -
关键词:
- 植物性饮食 /
- 植物性饮食指数 /
- 不健康的植物性饮食指数 /
- 老年人 /
- 死亡 /
- 中国老年健康和家庭幸福调查
Abstract:Objective To investigate the relationship between a plant-based diet and death in the elderly population. Methods Based on the data of the Chinese Longitudinal Healthy Longevity and Happy Family Study (CLHLS-HF), this study analyzed the follow-up survey data of 15 300 samples from 2008 to 2018. The plant-based diet index (PDI) and unhealthy plant-based diet index (UPDI) were used as indicators to evaluate the plant-based diet, which was grouped according to the quintile and divided into five groups: Q1, Q2, Q3, Q4, and Q5. A Cox survival analysis was used to construct a model to study the effects of PDI and UPDI on the death of individuals aged 65 years and above. Results After adjusting for confounding factors such as demographic characteristics, health behaviors, and underlying diseases, a statistically significant association was found between PDI and death (P < 0.001). Compared with Q1(control group), Q3 (HR=0.900, 95% CI: 0.832-0.974), Q4 (HR=0.872, 95% CI: 0.804-0.947), and Q5 (HR=0.779, 95% CI: 0.715-0.850) reduced the risk of death by 10.00%, 12.80%, 22.10%, respectively, while Q2 was not statistically significant. The UPDI was statistically associated with death (P < 0.001), with Q3 (HR=1.182, 95% CI: 1.080-1.294), Q4 (HR=1.206, 95% CI: 1.101-1.321), and Q5 (HR=1.210, 95% CI: 1.104-1.327) increased the risk of death by 18.20%, 20.60%, and 21.00%, respectively, compared with Q1. And Q2 was not statistically significant. With the increase in PDI, the mortality risk of the population showed a downward trend; with the decrease in UPDI score, the mortality risk of the population showed an upward trend (Ptrend < 0.001). Conclusion Based on the CLHLS-HF population, a reduced intake of plant foods, especially healthy ones, increases the mortality risk in the elderly. -

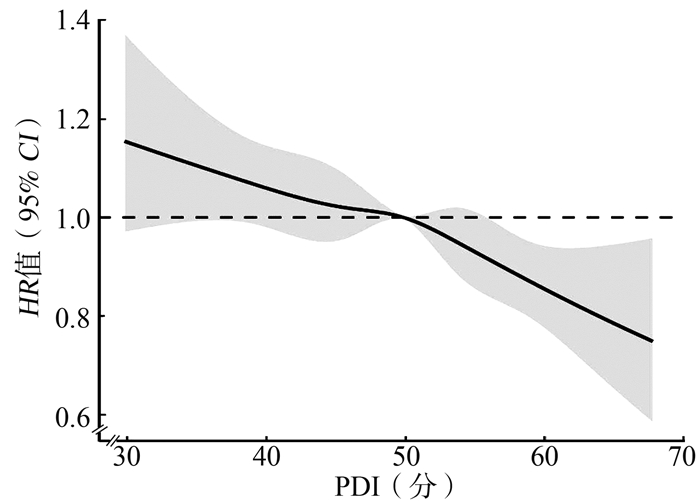
图 2 死亡风险随PDI的变化曲线:基于限制性立方样条
PDI:植物性饮食指数。
Figure 2. Change curve of death risk with PDI: based on restricted cubic spline

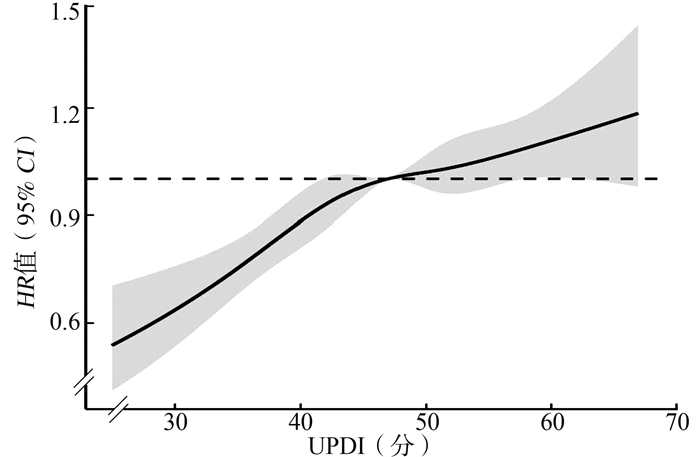
图 3 死亡风险随UPDI的变化曲线:基于限制性立方样条
UPDI:不健康的植物性饮食指数。
Figure 3. Change curve of death risk with UPDI: based on restricted cubic spline
表 1 研究对象基本特征(n=15 300)
Table 1. Basic characteristics of the study subject (n=15 300)
变量 人数(占比/%) PDI/分 UPDI/分 总分[M(P25, P75)] χ2值 P值 总分[M(P25, P75)] χ2值 P值 性别 122.599 < 0.001 275.212 < 0.001 女 8 879(58.03) 50(45, 54) 48(43, 52) 男 6 421(41.97) 50(46, 55) 46(41, 51) 年龄/岁 527.881 < 0.001 227.646 < 0.001 65~ < 85 5 422(35.44) 52(47, 56) 46(41, 51) ≥85 9 878(64.56) 49(45, 53) 48(43, 52) 城乡 194.374 < 0.001 1 337.652 < 0.001 农村 9 318(60.90) 50(45, 54) 49(44, 53) 城市 5 982(39.10) 50(46, 54) 45(40, 49) 地区 311.843 < 0.001 704.132 < 0.001 南方 10 915(71.34) 49(45, 54) 48(43, 53) 北方 4 385(28.66) 51(47, 55) 45(40, 49) 受教育水平 174.406 < 0.001 812.633 < 0.001 未接受过教育 9 838(64.30) 49(45, 54) 48(44, 53) 接受过教育 5 462(35.70) 51(46, 55) 45(40, 50) 婚姻状况① 324.792 < 0.001 481.136 < 0.001 无配偶 175(1.14) 50(46, 54) 49(44, 55) 有配偶 4 571(29.88) 51(47, 55) 46(41, 51) 丧偶 10 554(68.98) 49(45, 54) 48(43, 52) 是否吸烟① 218.098 < 0.001 234.191 < 0.001 是 2 543(16.62) 51(46, 55) 46(42, 51) 从不吸烟 10 349(67.64) 49(45, 54) 48(43, 52) 已戒烟 2 408(15.74) 50(46, 55) 46(41, 51) 是否喝酒① 186.404 < 0.001 220.783 < 0.001 是 2 537(16.58) 51(46, 55) 46(41, 50) 从不喝酒 10 679(69.80) 50(45, 54) 47(43, 52) 已戒酒 2 084(13.62) 50(46, 54) 47(42, 52) 是否参加体育锻炼 190.389 < 0.001 159.791 < 0.001 是 4 006(26.18) 51(47, 55) 44(40, 50) 否 11 294(73.82) 50(45, 54) 48(43, 52) 高血压② 2 966(19.39) 50(46, 54) 66.706 0.026 46(41, 51) 112.241 < 0.001 糖尿病② 381(2.49) 50(46, 54) 55.311 0.208 43(38, 47) 220.972 < 0.001 心脏病② 1 355(8.86) 51(47, 55) 67.070 0.042 45(40, 50) 231.382 < 0.001 中风及脑血管疾病② 921(6.02) 49(45, 53) 76.310 0.021 47(41, 52) 64.010 0.117 注:1. PDI:植物性饮食指数。2. UPDI:不健康的植物性饮食指数。
①婚姻状况、是否吸烟、是否喝酒在Cox分析中设置哑变量,分别以无配偶、从不吸烟、从不喝酒为对照组。②高血压、糖尿病、心脏病、中风及脑血管疾病的患病人数(患病率)。 下载: 导出CSV
下载: 导出CSV
表 2 PDI、UPDI与死亡关系的Cox回归模型
Table 2. Cox regression model of the relationship between PDI, UPDI and death
分组 模型1 ① 模型2 ② 模型3 ③ HR值(95% CI) P趋势值 HR值(95% CI) P趋势值 HR值(95% CI) P趋势值 PDI/分 Q1(<44) 1.000 1.000 1.000 Q2(44~<48) 0.906(0.838~0.978) 0.927(0.858~1.002) 0.929(0.859~1.004) Q3(48~<52) 0.832(0.769~0.900) 0.895(0.827~0.969) 0.900(0.832~0.974) Q4(52~<55) 0.728(0.672~0.790) 0.865(0.797~0.939) 0.872(0.804~0.947) Q5(≥55) 0.591(0.543~0.644) < 0.001 0.772(0.708~0.842) < 0.001 0.779(0.715~0.850) < 0.001 UPDI/分 Q1(<41) 1.000 1.000 1.000 Q2(41~<45) 1.199(1.095~1.312) 1.079(0.985~1.182) 1.084(0.989~1.187) Q3(45~<49) 1.370(1.255~1.496) 1.178(1.076~1.289) 1.182(1.080~1.294) Q4(49~<53) 1.410(1.293~1.539) 1.204(1.100~1.319) 1.206(1.101~1.321) Q5(≥53) 1.525(1.399~1.662) < 0.001 1.210(1.103~1.326) < 0.001 1.210(1.104~1.327) < 0.001 注:1. PDI:植物性饮食指数。2. UPDI:不健康的植物性饮食指数。
①未纳入混杂因素。②纳入年龄、性别、居住地、婚姻状况、受教育情况、吸烟、喝酒、体育锻炼。③调整人口学特征、健康行为、基础疾病。
下载: 导出CSV
表 3 65~ < 85岁人群中PDI、UPDI与死亡关系的Cox回归模型
Table 3. Cox regression model of the relationship between PDI, UPDI and death in people aged 65- < 85
分组 人数/例 模型1 ① 模型2 ② 模型3 ③ HR值(95% CI) P趋势值 HR值(95% CI) P趋势值 HR值(95% CI) P趋势值 PDI/分 Q1(< 44) 783 1.000 1.000 1.000 Q2(44~ < 48) 879 0.867(0.686~1.095) 0.901(0.712~1.139) 0.890(0.703~1.126) Q3(48~ < 52) 1 025 1.024(0.824~1.272) 1.076(0.864~1.338) 1.077(0.865~1.340) Q4(52~ < 55) 1 245 0.757(0.607~0.944) 0.812(0.649~1.016) 0.817(0.653~1.022) Q5(≥55) 1 490 0.641(0.514~0.799) < 0.001 0.692(0.553~0.865) < 0.001 0.707(0.565~0.884) 0.001 UPDI/分 Q1(< 41) 1 311 1.000 1.000 1.000 Q2(41~ < 45) 1 117 1.282(1.010~1.627) 1.171(0.920~1.490) 1.166(0.916~1.484) Q3(45~ < 49) 1 033 1.592(1.264~2.005) 1.390(1.096~1.763) 1.374(1.083~1.743) Q4(49~ < 53) 1 045 1.712(1.366~2.147) 1.409(1.112~1.786) 1.373(1.083~1.742) Q5(≥53) 916 2.129(1.703~2.662) < 0.001 1.647(1.294~2.096) < 0.001 1.606(1.262~2.044) < 0.001 注:1. PDI:植物性饮食指数。2. UPDI:不健康的植物性饮食指数。
①未纳入混杂因素。②纳入年龄、性别、居住地、婚姻状况、受教育情况、吸烟、喝酒、体育锻炼。③调整人口学特征、健康行为、基础疾病。
下载: 导出CSV
表 4 ≥85岁人群中PDI、UPDI与死亡关系的Cox回归模型
Table 4. Cox regression model of the relationship between PDI, UPDI and death in people ≥85 years old
分组 人数/例 模型1 ① 模型2 ② 模型3 ③ HR值(95% CI) P趋势值 HR值(95% CI) P趋势值 HR值(95% CI) P趋势值 PDI/分 Q1(< 44) 2 277 1.000 1.000 1.000 Q2(44~ < 48) 2 181 0.942(0.868~1.022) 0.932(0.858~1.012) 0.934(0.860~1.014) Q3(48~ < 52) 2 035 0.875(0.804~0.952) 0.869(0.798~0.946) 0.875(0.803~0.952) Q4(52~ < 55) 1 815 0.871(0.798~0.951) 0.879(0.804~0.960) 0.885(0.810~0.966) Q5(≥55) 1 570 0.792(0.721~0.870) < 0.001 0.798(0.726~0.877) < 0.001 0.803(0.730~0.882) < 0.001 UPDI/分 Q1(< 41) 1 749 1.000 1.000 1.000 Q2(41~ < 45) 1 943 1.083(0.982~1.194) 1.055(0.956~1.164) 1.059(0.960~1.169) Q3(45~ < 49) 2 027 1.177(1.071~1.295) 1.140(1.035~1.257) 1.145(1.038~1.262) Q4(49~ < 53) 2 015 1.216(1.107~1.337) 1.165(1.056~1.285) 1.167(1.057~1.288) Q5(≥53) 2 144 1.206(1.099~1.324) < 0.001 1.141(1.033~1.260) 0.003 1.143(1.035~1.262) 0.003 注:1. PDI:植物性饮食指数。2. UPDI:不健康的植物性饮食指数。
①未纳入混杂因素。②纳入年龄、性别、居住地、婚姻状况、受教育情况、吸烟、喝酒、体育锻炼。③调整人口学特征、健康行为、基础疾病。
下载: 导出CSV
-
[1] 唐乾敬. 新冠疫情提前拉响中国老龄化社会的警报[J]. 老龄科学研究, 2020, 8(5): 54-63. https://www.cnki.com.cn/Article/CJFDTOTAL-LLKX202005008.htmTang QJ. The COVID-19 pandemic has raised the alarm of population aging in China ahead of time[J]. Sci Res Aging, 2020, 8(5): 54-63. https://www.cnki.com.cn/Article/CJFDTOTAL-LLKX202005008.htm [2] Gibbs J, Gaskin E, Ji C, et al. The effect of plant-based dietary patterns on blood pressure: a systematic review and meta-analysis of controlled intervention trials[J]. J Hypertens, 2021, 39(1): 23-37. DOI: 10.1097/HJH.0000000000002604. [3] Yokoyama Y, Nishimura K, Barnard ND, et al. Vegetarian diets and blood pressure: a meta-analysis[J]. JAMA Intern Med, 2014, 174(4): 577-587. DOI: 10.1001/jamainternmed.2013.14547. [4] Dinu M, Abbate R, Gensini GF, et al. Vegetarian, vegan diets and multiple health outcomes: a systematic review with meta-analysis of observational studies[J]. Crit Rev Food Sci Nutr, 2017, 57(17): 3640-3649. DOI: 10.1080/10408398.2016.1138447. [5] Satija A, Bhupathiraju SN, Rimm EB, et al. Plant-based dietary patterns and incidence of type 2 diabetes in US men and women: results from three prospective cohort studies[J]. PLoS Med, 2016, 13(6): e1002039. DOI: 10.1371/journal.pmed.1002039. [6] Kuchakulla M, Nackeeran S, Blachman-Braun R, et al. The association between plant-based content in diet and testosterone levels in US adults[J]. World J Urol, 2021, 39(4): 1307-1311. DOI: 10.1007/s00345-020-03276-y. [7] 袁长征研究员团队发现中国老年人群健康植物性饮食模式与较低的死亡风险关联[J]. 浙江大学学报(医学版), 2022, 51(2): 174.Yuan Chang Zheng's research team found plant-based dietary patterns in relation to mortality among older adults in China[J]. J Zhejiang Univ (Med Sci), 2022, 51(2): 174. [8] 王璐, 阿丽亚·艾木都拉, 席苗苗, 等. 植物性饮食指数与代谢综合征及其组分的相关性研究[J]. 中国慢性病预防与控制, 2022, 30(3): 167-171. DOI: 10.16386/j.cjpccd.issn.1004-6194.2022.03.002.Wang L, Aliya AMDL, Xi MM, et al. Correlation between plant diet index and metabolic syndrome and its components[J]. Chin J Prevent Control Chronic Dis, 2022, 30(3): 167-171. DOI: 10.16386/j.cjpccd.issn.1004-6194.2022.03.002. [9] Mohammadifard N, Sajjadi F, Maghroun M, et al. Validation of a simplified food frequency questionnaire for the assessment of dietary habits in Iranian adults: Isfahan Healthy Heart Program, Iran. [J]. ARYA Atherosclerosis, 2015, 11(2): 139-146. [10] Wright N, Wilson L, Smith M, et al. The BROAD study: a randomised controlled trial using a whole food plant-based diet in the community for obesity, ischaemic heart disease or diabetes[J]. Nutr Diabetes, 2017, 7(3): e256. DOI: 10.1038/nutd.2017.3. [11] Dinu M, Abbate R, Gensini GF, et al. Vegetarian, vegan diets and multiple health outcomes: a systematic review with meta-analysis of observational studies[J]. Crit Rev Food Sci Nutr, 2017, 57(17): 3640-3649. DOI: 10.1080/10408398.2016.1138447. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 359
- HTML全文浏览量: 131
- PDF下载量: 48
- 被引次数: 0