

A prospective cohort study on the association between oral hygiene behaviors and the incidence of stroke
-
摘要:
目的 探讨贵州省人群口腔卫生行为与脑卒中发病的关系,为脑卒中的预防控制提供参考依据。 方法 采用分层随机整群抽样方法,2010年对抽取的贵州省12个县(市、区)18岁及以上常住居民共9 280人进行基线调查,于2016―2020年对该队列所有人群进行随访。运用SPSS 21.0软件进行数据分析,计量资料以(x±s)表示,多组间比较采用单因素方差分析。计数资料以构成比和率表示,组间比较采用χ2检验。采用Cox比例风险回归模型分析口腔卫生行为与脑卒中发病的关系,用Graphpad Prism 10.0.2软件绘制脑卒中发病风险森林图。 结果 最终纳入分析人群共7 970人,脑卒中发病204人,发病密度为3.62/1 000人年,多因素Cox回归分析结果显示,与每天刷牙1次以下的人群相比,每天刷牙1次可以降低34.3%的脑卒中发病风险(HR=0.657, 95% CI: 0.459~0.941),每天刷牙2次及以上可以降低50.8%的脑卒中发病风险(HR=0.492, 95% CI: 0.307~0.789)。每天刷牙2次及以上的人群缺血性脑卒中的发病风险是刷牙不足1次人群的0.515倍(HR=0.515, 95% CI: 0.298~0.891),口腔卫生行为与出血性脑卒中的发病无相关性。 结论 刷牙是脑卒中发病的保护性因素,每天刷牙2次及以上可以有效降低缺血性脑卒中的发病风险。 Abstract:Objective To explore the relationship between oral health behavior and the incidence of stroke in Guizhou Province, and to provide reference for the prevention and control of stroke. Methods A total of 9 280 permanent residents aged 18 years and above were selected using stratified random cluster sampling across 12 counties (cities and districts) in Guizhou Province in 2010. The cohort was followed up from 2016 to 2020. SPSS 21.0 software was used to analyze the data. The measured data were expressed as mean±standard deviation (x±s). One-way variance analysis was used for comparison among multiple groups. The count data were expressed as constituent ratio or rate. Chi-square test was used for comparison between groups. Cox proportional hazards regression model was used to analyze the relationship between oral hygiene behavior and stroke incidence. The Graphpad Prism 10.0.2 software was utilized for plotting stroke incidence risk. Results Of the 7 970 individuals included in the analysis, 204 experienced a stroke, with an incidence density of 3.62/1 000 person-years. The results of Cox regression analysis showed that compared with the individuals who brushed their teeth less than once a day, the risk of stroke decreased by 34.3% (HR=0.657, 95% CI: 0.459-0.941) for those brushing teeth once a day, and by 50.8% (HR=0.492, 95% CI: 0.307-0.789) for those brushing twice a day or more. The risk of ischemic stroke was 0.515-fold higher in those who brushed their teeth twice or more per day than in those who brushed less than once (HR=0.515, 95% CI: 0.298-0.891). However, no correlation was found between oral hygiene behavior and hemorrhagic stroke. Conclusions Brushing teeth is a protective factor for stroke. Brushing teeth twice or more every day can effectively reduce the risk of ischemic stroke. -
Key words:
- Oral hygiene behavior /
- Brushing frequency /
- Stroke /
- Cohort study
-

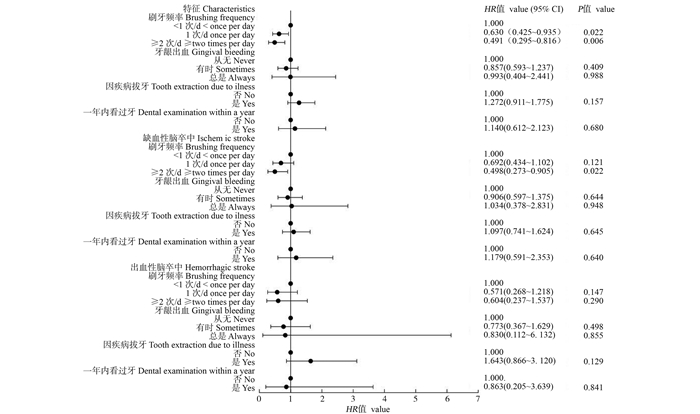
图 1 敏感性分析
调整年龄、性别、城乡、民族、婚姻状态和文化程度、油盐摄入过量、BMI、身体活动、吸烟、饮酒、每日蔬果摄入不足、基线高血压、糖尿病和血脂异常。
Figure 1. Sensitivity analysis
Adjusted age, gender, urban and rural areas, ethnicity, marital status and education, excessive oil and salt intake, BMI, physical activity, smoking, drinking, insufficient daily vegetable and fruit intake, baseline hypertension, diabetes and dyslipidemia.
表 1 基线情况
Table 1. Baseline characteristics
变量 Variable 刷牙频率① Brushing frequency ① t/χ2值
valueP值
value合计 Total
(n=7 970)<1次/d
<once per day
(n=1 032)1次/d
once per day
(n=4 729)≥2次/d ≥
two times per day
(n=2 209)年龄/岁 Age/years 44.50±15.15 55.86±15.01 44.02±14.15 40.23±14.66 420.105 <0.001 性别 Gender 40.740 <0.001 男 Male 3 791(47.57) 540(52.33) 2 322(49.10) 929(42.06) 女 Female 4 179(52.43) 492(47.67) 2 407(50.90) 1 280(57.94) 城乡 Urban and rural 185.443 <0.001 城市 Urban 2 650(33.25) 270(26.16) 1 392(29.44) 988(44.73) 农村 Rural 5 320(66.75) 762(73.84) 3 337(70.56) 1 221(55.27) 民族 Ethnicity 41.339 <0.001 少数民族 Ethnic minority 3 917(49.15) 559(54.17) 2 394(50.62) 964(43.64) 汉族 The Han nationality 4 053(50.85) 473(45.83) 2 335(49.38) 1 245(56.36) 婚姻状态 Marriage 93.949 <0.001 未婚/丧偶/独居/离婚 Unmarried/Widowed/Living alone/Divorced 1 536(19.27) 192(18.60) 768(16.24) 576(26.08) 已婚/同居 Married/cohabitation 6 434(80.73) 840(81.40) 3 961(83.76) 1 633(73.92) 文化程度 Education 792.688 <0.001 九年及以下≤9 years 6 924(86.88) 1 019(98.74) 4 358(92.15) 1547(70.03) 九年以上>9 years 1 046(13.12) 13(1.26) 371(7.85) 662(29.97) 油摄入过量 Excess oil intake 2.219 0.330 否 No 2 363(29.65) 303(29.36) 1 378(29.14) 682(30.87) 是 Yes 5 607(70.35) 729(70.64) 3 351(70.86) 1 527(69.13) 盐摄入过量 Excess salt intake 75.646 <0.001 否 No 2 268(28.46) 214(20.74) 1 288(27.24) 766(34.68) 是 Yes 5 702(71.54) 818(79.26) 3 441(72.76) 1 443(65.32) BMI/(kg·m-2) 22.89±3.36 22.31±3.24 22.90±3.35 23.11±3.41 20.322 <0.001 总活动时间过少 Less total physical activity time 50.852 <0.001 否 No 5 956(74.73) 773(74.90) 3 653(77.25) 1 530(69.26) 是 Yes 2 014(25.27) 259(25.10) 1 076(22.75) 679(30.74) 饮酒 Drinking 15.837 <0.001 否 No 5 406(67.83) 652(63.18) 3 277(69.30) 1 477(66.86) 是 Yes 2 564(32.17) 380(36.82) 1 452(30.70) 732(33.14) 吸烟 Smoking 15.935 <0.001 否 No 7 537(94.57) 1 002(97.09) 4 464(94.40) 2 071(93.75) 是 Yes 433(5.43) 30(2.91) 265(5.60) 138(6.25) 每日蔬果摄入不足 Insufficient daily intake of fruits and vegetables 103.871 <0.001 否 No 3 889(48.97) 352(34.17) 2 418(51.34) 1 119(50.84) 是 Yes 4 052(51.03) 678(65.83) 2 292(48.66) 1 082(49.16) 高血压 Hypertension 53.603 <0.001 否 No 5 890(73.90) 667(64.63) 3 545(74.96) 1 678(75.96) 是 Yes 2 080(26.10) 365(35.37) 1 184(25.04) 531(24.04) 糖尿病② Diabetes ② 10.683 0.005 否 No 6 535(82.17) 810(78.56) 3 896(82.58) 1 829(82.99) 是 Yes 1 418(17.83) 221(21.44) 822(17.42) 375(17.01) 血脂异常② Dyslipidemia ② 28.612 <0.001 否 No 2 058(27.38) 312(31.87) 1 249(28.30) 497(23.41) 是 Yes 5 458(72.62) 667(68.13) 3 165(71.70) 1 626(76.59) 牙龈出血② Gingival bleeding ② 73.244 <0.001 从无 Never 5 479(68.82) 808(78.37) 3 267(69.16) 1 404(63.64) 有时 Sometimes 2 240(28.14) 205(19.88) 1 319(27.92) 716(32.46) 总是 Always 242(3.04) 18(1.75) 138(2.92) 86(3.90) 因疾病拔牙② Tooth extraction due to illness ② 163.931 <0.001 否 No 5 949(75.45) 596(59.24) 3 640(77.56) 1 713(78.36) 是 Yes 1 936(24.55) 410(40.76) 1 053(22.44) 473(21.64) 一年内看过牙② Dental examination within a year ② 54.897 <0.001 否 No 7 610(95.59) 992(96.59) 4 570(96.66) 2 048(92.84) 是 Yes 351(4.41) 35(3.41) 158(3.34) 158(7.16) 注:BMI, 体质指数。
① 以[人数(占比/%)]表示;② 表示该变量有缺失值
Note: BMI, body mass index.
① [Number of people (proportion/%)]; ② Indicates that the variable has a missing value. 下载: 导出CSV
下载: 导出CSV
表 2 口腔卫生行为与脑卒中发病的Cox回归分析
Table 2. Cox regression analysis of oral hygiene behavior and stroke incidence
特征 Characteristics 发病人数/调查人数
Number of patients/survey Total发病密度
(1 000人年)
Incidence density
(1 000PYs)未调整模型
Unadjusted model模型1 ① Model 1① 模型2 ② Model 2 ② 模型3 ③ Model 3 ③ HR值 value
(95% CI)P值
valueHR值 value
(95% CI)P值
valueHR值 value
(95% CI)P值
valueHR值 value
(95% CI)P值
value刷牙频率 Brushing frequency <1次/d<Once per day 51/1 032 7.41 1.000 1.000 1.000 1.000 1次/d Once per day 112/4 729 3.35 0.430
(0.308~0.599)<0.001 0.697
(0.491~0.989)0.043 0.683
(0.478~0.975)0.036 0.657
(0.459~0.941)0.022 ≥2次/d ≥Two times per day 41/2 209 2.56 0.319
(0.211~0.482)<0.001 0.547
(0.345~0.868)0.010 0.559
(0.351~0.891)0.014 0.492
(0.307~0.789)0.003 P趋势值Ptrend value <0.001 0.010 0.014 0.003 牙龈出血 Gingival bleeding 从无 Never 147/5 479 3.83 1.000 1.000 1.000 1.000 有时 Sometimes 49/2 240 3.03 0.795
(0.576~1.099)0.166 0.964
(0.695~1.337)0.826 0.971
(0.700~1.347)0.861 0.971
(0.697~1.352)0.860 总是 Always 8/242 4.71 1.218
(0.598~2.482)0.587 1.470
(0.717~3.010)0.293 1.444
(0.705~2.960)0.315 1.256
(0.585~2.696)0.559 P趋势值Ptrend value 0.445 0.679 0.670 0.847 因疾病拔牙 Tooth extraction due to illness 否 No 126/5 949 2.96 1.000 1.000 1.000 1.000 是 Yes 75/1 936 5.67 1.960
(1.472~2.609)<0.001 1.227
(0.907~1.660)0.184 1.195
(0.882~1.619)0.251 1.207
(0.888~1.640)0.229 P趋势值Ptrend value <0.001 0.184 0.251 0.229 一年内看过牙 Dental examination within a year 否 No 188/7 610 3.49 1.000 1.000 1.000 1.000 是 Yes 15/351 6.23 1.778
(1.051~3.009)0.032 1.473
(0.864~2.509)0.154 1.391
(0.815~2.373)0.226 1.365
(0.798~2.335)0.255 P趋势值Ptrend value 0.032 0.154 0.226 0.255 注:①调整年龄、性别、城乡、民族、婚姻状态和文化程度。②在模型1基础上调整油盐摄入过量、BMI、身体活动、吸烟、饮酒、每日蔬果摄入不足。③在模型2基础上调整基线高血压、糖尿病和血脂异常。
Note: ① Adjust age, gender, urban and rural areas, ethnicity, marital status and educational level. ② Regulating excessive oil and salt intake, BMI, physical activity, smoking, drinking and insufficient daily vegetable and fruit intake on the basis of model 1. ③ Adjust baseline hypertension, diabetes and dyslipemia on the basis of model 2.
下载: 导出CSV
表 3 口腔卫生行为与脑卒中亚型发病的Cox回归分析
Table 3. Cox regression analysis of oral hygiene behavior and incidence of stroke subtype
特征 Characteristics 发病人数
Number of patients发病密度
(1 000人年)
Incidence density
(1 000PYs)未调整模型
Unadjusted model模型1 ① Model 1① 模型2 ② Model 2 ② 模型3 ③ Model 3 ③ HR值 value
(95% CI)P值
valueHR值 value
(95% CI)P值
valueHR值 value
(95% CI)P值
valueHR值 value
(95% CI)P值
value出血性脑卒中 Hemorrhagic stroke 刷牙频率 Brushing frequency <1次/d<Once per day 15 2.18 1.000 1.000 1.000 1.000 1次/d Once per day 30 0.90 0.389
(0.209~0.725)0.003 0.672
(0.350~1.292)0.233 0.688
(0.355~1.330)0.266 0.625
(0.319~1.224)0.171 ≥2次/d ≥Two times per day 14 0.87 0.362
(0.174~0.753)0.007 0.777
(0.348~1.732)0.537 0.809
(0.358~1.825)0.609 0.658
(0.285~1.519)0.327 P趋势值Ptrend value 0.014 0.548 0.617 0.327 牙龈出血 Gingival bleeding 从无 Never 41 1.07 1.000 1.000 1.000 1.000 有时 Sometimes 14 0.86 0.816
(0.445~1.498)0.513 0.981
(0.532~1.812)0.952 1.007
(0.545~1.862)0.982 1.012
(0.535~1.915)0.971 总是 Always 4 2.35 2.172
(0.778~6.065)0.139 2.953
(1.043~8.358)0.041 3.018
(1.065~8.553)0.038 2.348
(0.714~7.715)0.160 P趋势值Ptrend value 0.713 0.276 0.239 0.420 因疾病拔牙 Tooth extraction due to illness 否 No 36 0.85 1.000 1.000 1.000 1.000 是 Yes 21 1.59 1.908
(1.113~3.269)0.019 1.210
(0.687~2.131)0.508 1.218
(0.688~2.156)0.499 1.284
(0.717~2.299)0.400 P趋势值Ptrend value 0.019 0.508 0.499 0.400 一年内看过牙 Dental examination within a year 否 No 56 1.04 1.000 1.000 1.000 1.000 是 Yes 3 1.25 1.184
(0.371~3.783)0.776 1.083
(0.335~3.506)0.894 1.085
(0.334~3.522)0.892 1.096
(0.336~3.577)0.880 P趋势值Ptrend value 0.776 0.894 0.892 0.880 缺血性脑卒中 Ischemic stroke 刷牙频率 Brushing frequency <1次/d<Once per day 36 5.24 1.000 1.000 1.000 1.000 1次/d Once per day 85 2.54 0.463
(0.314~0.685)<0.001 0.755
(0.500~1.139)0.180 0.724
(0.476~1.102)0.132 0.712
(0.467~1.086)0.115 ≥2次/d ≥Two times per day 31 1.94 0.345
(0.213~0.558)<0.001 0.564
(0.328~0.968)0.038 0.561
(0.325~0.968)0.038 0.515
(0.298~0.891)0.018 P趋势值Ptrend value <0.001 0.037 0.038 0.018 牙龈出血 Gingival bleeding 从无 Never 108 2.82 1.000 1.000 1.000 1.000 有时 Sometimes 38 2.35 0.841
(0.581~1.218)0.360 1.029
(0.708~1.495)0.882 1.020
(0.702~1.482)0.918 1.027
(0.706~1.495)0.889 总是 Always 6 3.53 1.247
(0.548~2.836)0.599 1.448
(0.632~3.316)0.381 1.405
(0.613~3.218)0.422 1.389
(0.606~3.180)0.437 P趋势值Ptrend value 0.682 0.546 0.596 0.585 因疾病拔牙 Tooth extraction due to illness 否 No 96 2.26 1.000 1.000 1.000 1.000 是 Yes 54 4.08 1.853
(1.327~2.587)<0.001 1.130
(0.794~1.607)0.497 1.091
(0.767~1.554)0.627 1.083
(0.759~1.546)0.659 P趋势值Ptrend value <0.001 0.497 0.627 0.659 一年内看过牙 Dental examination within a year 否 No 138 2.56 1.000 1.000 1.000 1.000 是 Yes 13 5.40 2.103
(1.191~3.714)0.010 1.668
(0.937~2.969)0.082 1.534
(0.860~2.736)0.147 1.490
(0.833~2.664)0.179 P趋势值Ptrend value 0.010 0.082 0.147 0.179 注:①调整年龄、性别、城乡、民族、婚姻状态和文化程度。②在模型1基础上调整油盐摄入过量、BMI、身体活动、吸烟、饮酒、每日蔬果摄入不足。③在模型2基础上调整基线高血压、糖尿病和血脂异常。
Note: ① Adjust age, gender, urban and rural areas, ethnicity, marital status and educational level. ② Regulating excessive oil and salt intake, BMI, physical activity, smoking, drinking and insufficient daily vegetable and fruit intake on the basis of model 1. ③ Adjust baseline hypertension, diabetes and dyslipemia on the basis of model 2.
下载: 导出CSV
-
[1] Venketasubramanian N, Yoon BW, Pandian J, et al. Stroke epidemiology in south, east, and south-east Asia: a review[J]. J Stroke, 2017, 19(3): 286-294. DOI: 10.5853/jos.2017.00234. [2] 2019 Stroke Collaborators GBD. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet Neurol, 2021, 20(10): 795-820. DOI: 10.1016/S1474-4422(21)00252-0. [3] 《中国脑卒中防治报告》编写组. 《中国脑卒中防治报告2020》概要[J]. 中国脑血管病杂志, 2022, 19(2): 136-144. DOI: 10.3969/j.issn.1672-5921.2022.02.011.The Writing Committee of the Report on Stroke Prevention and Treatment in China. Brief report on stroke prevention and treatment in China, 2020[J]. Chin J Cerebrovasc Dis, 2022, 19(2): 136-144. DOI: 10.3969/j.issn.1672-5921.2022.02.011. [4] Libby P. Inflammation and cardiovascular disease mechanisms[J]. Am J Clin Nutr, 2006, 83(2): 456S-460S. DOI: 10.1093/ajcn/83.2.456S. [5] Rahimi A, Afshari Z. Periodontitis and cardiovascular disease: a literature review[J]. ARYA Atheroscler, 2021, 17(5): 1-8. DOI: 10.22122/arya.v17i0.2362. [6] Rydén L, Buhlin K, Ekstrand E, et al. Periodontitis increases the risk of a first myocardial infarction: a report from the Parokrank study[J]. Circulation, 2016, 133(6): 576-583. DOI: 10.1161/CIRCULATIONAHA.115.020324. [7] Kuwabara M, Motoki Y, Ichiura K, et al. Association between toothbrushing and risk factors for cardiovascular disease: a large-scale, cross-sectional Japanese study[J]. BMJ Open, 2016, 6(1): e009870. DOI: 10.1136/bmjopen-2015-009870. [8] Carrizales-Sepúlveda EF, Ordaz-Farías A, Vera-Pineda R, et al. Periodontal disease, systemic inflammation and the risk of cardiovascular disease[J]. Heart Lung Circ, 2018, 27(11): 1327-1334. DOI: 10.1016/j.hlc.2018.05.102. [9] Wang Y, Jiang Y, Chen Y, et al. Associations of oral hygiene with incident hypertension and type 2 diabetes mellitus: a population based cohort study in Southwest China[J]. J Clin Hypertens (Greenwich), 2022, 24(4): 483-492. DOI: 10.1111/jch.14451. [10] Cao L, Zhou J, Chen Y, et al. Effects of body mass index, waist circumference, waist-to-height ratio and their changes on risks of dyslipidemia among Chinese adults: the Guizhou population health cohort study[J]. Int J Environ Res Public Health, 2021, 19(1): 341. DOI: 10.3390/ijerph19010341. [11] Chang Y, Woo HG, Lee JS, et al. Better oral hygiene is associated with lower risk of stroke[J]. J Periodontol, 2021, 92(1): 87-94. DOI: 10.1002/JPER.20-0053. [12] de Oliveira C, Watt R, Hamer M. Toothbrushing, inflammation, and risk of cardiovascular disease: results from Scottish Health Survey[J]. BMJ, 2010, 340: c2451. DOI: 10.1136/bmj.c2451. [13] Chapple IL, Van der Weijden F, Doerfer C, et al. Primary prevention of periodontitis: managing gingivitis[J]. J Clin Periodontol, 2015, 42(Suppl 16): S71-S76. DOI: 10.1111/jcpe.12366. [14] Tribble GD, Lamont RJ. Bacterial invasion of epithelial cells and spreading in periodontal tissue[J]. Periodontol 2000, 2010, 52(1): 68-83. DOI: 10.1111/j.1600-0757.2009.00323.x. [15] Pizzo G, Guiglia R, Lo Russo L, et al. Dentistry and internal medicine: from the focal infection theory to the periodontal medicine concept[J]. Eur J Intern Med, 2010, 21(6): 496-502. DOI: 10.1016/j.ejim.2010.07.011. [16] Baniulyte G, Piela K, Culshaw S. How strong is the link between periodontitis and stroke?[J]. Evid Based Dent, 2021, 22(1): 10-11. DOI: 10.1038/s41432-021-0161-7. [17] 杜芹, 马歆茹. 牙周致病菌与系统性疾病的相关性研究进展[J]. 南方医科大学学报, 2020, 40(5): 759-764. DOI: 10.12122/j.issn.1673-4254.2020.05.24.Du Q, Ma XR. Research progress of correlation between periodontal pathogens and systemic diseases[J]. J South Med Univ, 2020, 40(5): 759-764. DOI: 10.12122/j.issn.1673-4254.2020.05.24. [18] Passoja A, Puijola I, Knuuttila M, et al. Serum levels of interleukin-10 and tumour necrosis factor-α in chronic periodontitis[J]. J Clin Periodontol, 2010, 37(10): 881-887. DOI: 10.1111/j.1600-051X.2010.01602.x. [19] Gani DK, Mallineni SK, Ambalavanan, et al. Estimation of the levels of C-reactive protein, interleukin-6, total leukocyte count, and differential count in peripheral blood smear of patients with chronic periodontitis in a South Indian population[J]. West Indian Med J, 2012, 61(8): 826-831. [20] Pejcic A, Kesic LJ, Milasin J. C-reactive protein as a systemic marker of inflammation in periodontitis[J]. Eur J Clin Microbiol Infect Dis, 2011, 30(3): 407-414. DOI: 10.1007/s10096-010-1101-1. [21] Esenwa CC, Elkind MS. Inflammatory risk factors, biomarkers and associated therapy in ischaemic stroke[J]. Nat Rev Neurol, 2016, 12(10): 594-604. DOI: 10.1038/nrneurol.2016.125. [22] Kobayashi D, Mizuno A, Mitsui R, et al. Frequency of daily tooth brushing and subsequent cardiovascular events[J]. Coron Artery Dis, 2020, 31(6): 545-549. DOI: 10.1097/MCA.0000000000000882. [23] Jimenez M, Krall EA, Garcia RI, et al. Periodontitis and incidence of cerebrovascular disease in men[J]. Ann Neurol, 2009, 66(4): 505-512. DOI: 10.1002/ana.21742. [24] Cai G, Cai G, Zhou H, et al. Mesenchymal stem cell-derived exosome miR-542-3p suppresses inflammation and prevents cerebral infarction[J]. Stem Cell Res Ther, 2021, 12(1): 2. DOI: 10.1186/s13287-020-02030-w. [25] Sanz M, Marco Del Castillo A, Jepsen S, et al. Periodontitis and cardiovascular diseases: consensus report[J]. J Clin Periodontol, 2020, 47(3): 268-288. DOI: 10.1111/jcpe.13189. [26] Park SY, Kim SH, Kang SH, et al. Improved oral hygiene care attenuates the cardiovascular risk of oral health disease: a population-based study from Korea[J]. Eur Heart J, 2019, 40(14): 1138-1145. DOI: 10.1093/eurheartj/ehy836. [27] Pietropaoli D, Monaco A, D'Aiuto F, et al. Active gingival inflammation is linked to hypertension[J]. J Hypertens, 2020, 38(10): 2018-2027. DOI: 10.1097/HJH.0000000000002514. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 470
- HTML全文浏览量: 146
- PDF下载量: 38
- 被引次数: 0