

-
摘要:
目的 探讨上海市松江区居民生活方式对脑卒中风险的影响在不同年龄段中是否存在差异。 方法 选取上海郊区自然人群队列和生物样本库中松江区的31 771名研究对象,计算其健康生活方式评分(包括不吸烟、积极体育锻炼、均衡膳食和正常体重),并随访至2021年12月31日。分别采用Cox比例风险回归和泊松回归评估不同基线年龄组和暴露年龄组中不同的生活方式或健康生活方式评分与新发脑卒中的HR值(95% CI)和RR值(95% CI)。基线年龄分层:年轻组(20~<62岁)、中年组(62~<68岁)以及老年组(≥68岁)。暴露年龄分层:年轻组(20~<65岁)、中年组(65~<70岁)以及老年组(≥70岁)。 结果 在5.0年的中位随访时间内共新发488例脑卒中事件。控制混杂变量后,两种方法都未发现不吸烟、积极体育锻炼、均衡膳食和正常体重与脑卒中发病风险的关联在不同的年龄组有显著差异。与基线生活方式评分≤1分组相比,年轻组、中年组及老年组中评分≥3分组的新发脑卒中风险较低(HR=0.67, 95% CI: 0.43~1.03, P=0.072; HR=0.59, 95% CI: 0.39~0.91, P=0.015; HR=0.64, 95% CI: 0.42~1.00, P=0.043和RR=0.63, 95% CI: 0.42~0.96, P=0.028; RR =0.61, 95% CI: 0.40~0.94, P=0.023; RR=0.63, 95% CI: 0.40~0.99, P=0.045)。 结论 在上海市松江区居民中没有发现不同的生活方式与脑卒中的关联存在年龄差异。提示在任何年龄阶段都应重视健康的生活方式。当整体的生活方式比较健康时可大幅度降低脑卒中发病风险。 Abstract:Objective To investigate whether there are differences in the influence of lifestyle on stroke risk in different age groups in Songjiang district of Shanghai. Methods A total of 31 771 study participants from the Songjiang District in the Shanghai Suburban Adult Cohort and Biobank were selected to calculate their healthy lifestyle scores (including non-smoking, active physical activity, balanced diet, and normal body weight) and were followed until December 31, 2021. Cox proportional risk regression and Poisson regression were used to determine the HR (95% CI) and RR (95% CI) of different lifestyle or healthy lifestyle scores associated with stroke in various baseline age groups and exposed age groups, respectively. Baseline age was stratified by young (20- < 62 years), middle (62- < 68 years), and old (≥68 years) groups. Exposure age was stratified by young (20- < 65 years), middle (65- < 70 years), and old (≥70 years) groups. Results Over a median follow-up of 5.0 years, 488 participants developed stroke. After adjusting confounding factors, the associations between non-smoking, active physical activity, balanced diet, or normal body weight and the risk of stroke were not significantly different across age groups, regardless of the method used. The risk of stroke was lower in the group with a score of ≥3 in the young, middle, and old stratum compared with the group with a baseline lifestyle score ≤1 (HR=0.67, 95% CI: 0.43-1.03, P=0.072; HR=0.59, 95% CI: 0.39-0.91, P=0.015; HR=0.64, 95% CI: 0.42-1.00, P=0.043; RR=0.63, 95% CI: 0.42-0.96, P=0.028; RR=0.61, 95% CI: 0.40-0.94, P=0.023; RR=0.63, 95% CI: 0.40-0.99, P=0.045). Conclusions No age-related differences in the association of different lifestyles with stroke are found among residents of Songjiang District, Shanghai. It implies that a healthy lifestyle should be emphasized regardless of age. In addition, a healthy lifestyle can substantially reduce the risk of stroke. -
Key words:
- Stroke /
- Lifestyle /
- Age difference /
- Cohort study
-

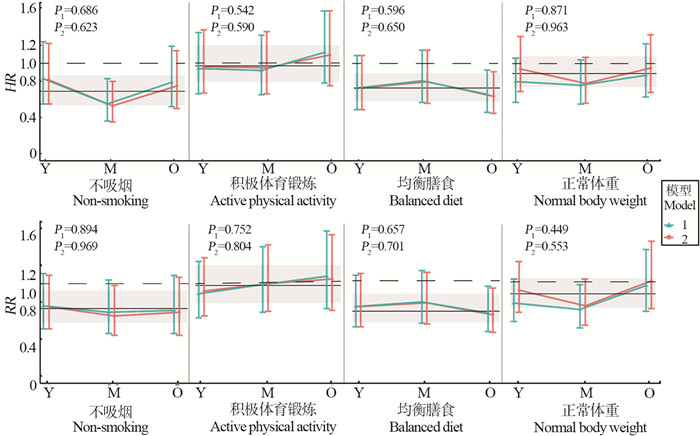
图 1 不同年龄段中不同健康生活方式与脑卒中风险的关联
Cox比例风险回归和泊松回归分别评估了各年龄组(年轻组:Y,中年组:M,老年组:O)中的不同健康生活方式与脑卒中的HR及RR值。模型1调整了年龄和性别(绿色表示)。模型2调整年龄、性别、受教育年限、婚姻状况、脑卒中家族史、是否有高血压、糖尿病或高脂血症病史(红色表示)。黑色实线为在整个年龄阶段中通过多变量调整的HR或RR值,阴影部分为95% CI。
Figure 1. The association of various healthy lifestyles with the risk of stroke in different age groups
Cox proportional risk regression and Poisson regression were used to assess the HR and RR for stroke by different healthy lifestyles in each age group (young: Y, middle: M, and old: O), respectively. Model 1 adjusts for age and sex (indicated in green). Model 2 adjusts for age, sex, years of education, marital status, family history of stroke, and whether there is a history of hypertension, diabetes or hyperlipidemia (indicated in red). The solid black line is the HR or RR adjusted by multivariate adjustment throughout the age range, and the shaded area is the 95% CI.
表 1 基线研究对象中有无发生脑卒中的人口学基本特征
Table 1. Characteristics of study participants according to stroke at baseline
特征Feature 总人群① Total ① (n=31 771) 发生脑卒中① Stroke ① (n=488) 未发生脑卒中① Non-stroke ① (n=31 283) P值value 年龄/岁Age/years 55.48±11.28 62.92±7.64 55.36±11.29 < 0.001 女性Female 18 882(59.43) 203(41.59) 18 679(59.71) < 0.001 受教育年限/年Years of education/years < 0.001 ≤6 14 221(44.76) 307(62.91) 13 914(44.48) 7~<12 15 310(48.19) 174(35.66) 15 136(48.38) ≥12 2 240(7.05) 7(1.43) 2 233(7.14) 未婚Unmarried 2 199(6.92) 35(7.17) 2 164(6.92) 0.897 健康生活方式Healthy lifestyle 不吸烟Non-smoking 25 259(79.50) 326(66.80) 24 933(79.70) < 0.001 积极体育锻炼Active physical activity 7 795(24.53) 119(24.39) 7 676(24.54) 0.980 均衡膳食Balanced diet 27 013(85.02) 371(76.02) 26 642(85.16) < 0.001 正常体重Normal body weight 14 377(45.25) 177(36.27) 14 200(45.39) < 0.001 健康生活方式评分/分Healthy lifestyle score/score < 0.001 ≤1 4 854(15.28) 131(26.84) 4 723(15.10) 2 12 641(39.79) 209(42.83) 12 432(39.74) ≥3 14 276(44.93) 148(30.33) 14 128(45.16) 高血压Hypertention 16 051(50.52) 359(73.57) 15 692(50.16) < 0.001 糖尿病Diabetes 4 281(13.47) 150(30.74) 4 131(13.21) < 0.001 高脂血症Hyperlipidaemia 10 077(31.72) 203(41.60) 9 874(31.56) < 0.001 脑卒中家族史Family history of stroke 2 182(6.87) 31(6.35) 2 151(6.88) 0.716 注:①以人数(占比/%)或x±s表示。
Note: ① Number of people(proportion/%) or x±s 下载: 导出CSV
下载: 导出CSV
表 2 每个年龄层的患病人数、暴露年数、脑卒中事件数量和粗脑卒中发生率的描述
Table 2. Description of the number of patients, years of exposure, number of stroke events, and crude stroke rates within each age stratum
特征Feature 基线年龄分析/岁Analysis relative to age at baseline/years 暴露年龄分析/岁Analysis relative to age at exposure/years 20~<62 62~<68 ≥68 20~<65 65~<70 ≥70 总人群Total 20 837 6 679 4 255 随访中位时间/年Median follow-up/years 5.1 4.6 4.6 脑卒中Strokes 人数Number of people 170 170 148 占比/% Proportion/% (95% CI) 0.82 (0.71~0.95) 2.55 (2.20~2.96) 3.48 (2.97~4.07) 随访人年Person-years of follow-up 120 757 52 147 27 424 脑卒中事件数Stroke events 188 165 135 脑卒中发病率/10万人年Incidence of stroke per 100 000 person-years (95% CI) 155.69 (134.95~179.61) 316.41 (271.64~368.57) 492.26 (415.85~582.72) 注:每个人在每个年龄层内对风险年数的贡献被计算为参与者在不同年龄层内的潜在年龄。
Notes: Each person′s contribution to years at risk within each age stratum was calculate as the participant potentially ages between age strata.
下载: 导出CSV
表 3 健康生活方式评分与脑卒中的风险比及相对风险
Table 3. Hazard ratio and relative risk for stroke by healthy lifestyle score
年龄组Age group 健康生活方式评分Healthy lifestyle score HR值value (95% CI) 健康生活方式评分Healthy lifestyle score RR值value(95% CI) ≤1 2 ≥3 P趋势 Ptrend ≤1 2 ≥3 P趋势 Ptrend Y 模型1 Model 1 1.00 0.70(0.47~1.03) 0.56(0.37~0.87) 0.011 1.00 0.73(0.51~1.06) 0.54(0.35~0.81) 0.003 模型2 Model 2 1.00 0.74(0.50~1.08) 0.67(0.43~1.03) 0.080 1.00 0.77(0.54~1.12) 0.63(0.42~0.96) 0.033 M 模型1 Model 1 1.00 0.74(0.51~1.08) 0.57(0.37~0.87) 0.009 1.00 0.77(0.52~1.13) 0.59(0.39~0.91) 0.017 模型2 Model 2 1.00 0.76(0.52~1.10) 0.59(0.39~0.91) 0.016 1.00 0.77(0.53~1.14) 0.61(0.40~0.94) 0.027 O 模型1 Model 1 1.00 0.74(0.50~1.11) 0.63(0.41~0.98) 0.047 1.00 0.67(0.44~1.03) 0.62(0.39~0.97) 0.046 模型2 Model 2 1.00 0.76(0.51~1.14) 0.64(0.42~1.00) 0.050 1.00 0.69(0.45~1.05) 0.63(0.40~0.99) 0.050 注:1. Cox比例风险回归和泊松回归分别评估了各年龄组(年轻组:Y,中年组:M,老年组:O)中的健康生活方式评分与脑卒中的HR及RR值。
2. 模型1调整了年龄和性别; 模型2调整年龄、性别、受教育年限、婚姻状况、脑卒中家族史、是否有高血压、糖尿病或高脂血症病史。
Notes:1. Cox proportional risk regression and Poisson regression were used to assess the HR and RR for stroke by healthy lifestyles score in each age group (young: Y, middle: M, and old: O), respectively.
2. Model 1 adjusts for age and sex. Model 2 adjusts for age, sex, years of education, marital status, family history of stroke, and whether there is a history of hypertension, diabetes or hyperlipidemia.
下载: 导出CSV
-
[1] GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1789-1858. DOI: 10.1016/S0140-6736(18)32279-7. [2] Wang W, Jiang B, Sun H, et al. Prevalence, incidence, and mortality of stroke in China: Results from a nationwide population-based survey of 480 687 adults[J]. Circulation, 2017, 135(8): 759-771. DOI: 10.1161/CIRCULATIONAHA.116.025250. [3] 2016 Lifetime Risk of Stroke Collaborators GBD, Feigin VL, Nguyen G, et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016[J]. N Engl J Med, 2018, 379(25): 2429-2437. DOI: 10.1056/NEJMoa1804492. [4] Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2022 update: a report from the american heart association[J]. Circulation, 2022, 145(8): e153-e639. DOI: 10.1161/cir.0000000000001074. [5] Rigotti NA, Clair C. Managing tobacco use: the neglected cardiovascular disease risk factor[J]. Eur Heart J, 2013, 34(42): 3259-3267. DOI: 10.1093/eurheartj/eht352. [6] Preventive Services Task Force US, Krist AH, Davidson KW, et al. Behavioral counseling interventions to promote a healthy diet and physical activity for cardiovascular disease prevention in adults with cardiovascular risk factors: US Preventive Services Task force recommendation statement[J]. JAMA, 2020, 324(20): 2069-2075. DOI: 10.1001/jama.2020.21749. [7] Khan SS, Ning H, Wilkins JT, et al. Association of body mass index with lifetime risk of cardiovascular disease and compression of morbidity[J]. JAMA Cardiol, 2018, 3(4): 280-287. DOI: 10.1001/jamacardio.2018.0022. [8] Han Y, Hu Y, Yu C, et al. Lifestyle, cardiometabolic disease, and multimorbidity in a prospective Chinese study[J]. Eur Heart J, 2021, 42(34): 3374-3384. DOI: 10.1093/eurheartj/ehab413. [9] 顾东风, 翁建平, 鲁向锋. 中国健康生活方式预防心血管代谢疾病指南[J]. 中国循环杂志, 2020, 35(3): 209-230. DOI: 10.3969/j.issn.1000-3614.2020.03.001.Gu DF, Weng JP, Lu XF. Chinese guideline on healthy lifestyle to prevent cardiometabolic diseases[J]. Chin Circul J, 2020, 35(3): 209-230. DOI: 10.3969/j.issn.1000-3614.2020.03.001. [10] 赵琦, 刘星, 姜永根, 等. 上海郊区自然人群队列和生物样本库建设[J]. 中华流行病学杂志, 2023, 44(1): 22-33. DOI: 10.3760/cma.j.cn112338-20221018-00888.Zhao Q, Liu X, Jiang YG, et al. Establishment of Shanghai suburban adult cohort and biobank[J]. Chin J Epidemiol, 2023, 44(1): 28-33. DOI: 10.3760/cma.j.cn112338-20221018-00888. [11] 唐敏华, 崔淑衡, 易康祺, 等. 上海市松江区社区脑卒中人群共病现状研究[J]. 上海预防医学, 2022, 34(9): 888-894. DOI: 10.19428/j.cnki.sjpm.2022.21999.Tang MH, Cui SH, Yi KQ, et al. Cross-sectional study on comorbidities in community patients with stroke in Songjiang District, Shanghai[J]. Shanghai Journal of Preventive Medicine, 2022, 34(9): 888-894. DOI: 10.19428/j.cnki.sjpm.2022.21999. [12] Burns DM. Epidemiology of smoking-induced cardiovascular disease[J]. Prog Cardiovasc Dis, 2003, 46(1): 11-29. DOI: 10.1016/s0033-0620(03)00079-3. [13] Howard G, Banach M, Kissela B, et al. Age-related differences in the role of risk factors for ischemic stroke[J]. Neurology, 2023, 100(14): e1444-e1453. DOI: 10.1212/WNL.0000000000206837. [14] Abbott RD, Curb JD, Rodriguez BL, et al. Age-related changes in risk factor effects on the incidence of thromboembolic and hemorrhagic stroke[J]. J Clin Epidemiol, 2003, 56(5): 479-486. DOI: 10.1016/s0895-4356(02)00611-x. [15] Shan Z, Li Y, Baden MY, et al. Association between healthy eating patterns and risk of cardiovascular disease[J]. JAMA Intern Med, 2020, 180(8): 1090-1100. DOI: 10.1001/jamainternmed.2020.2176. [16] Psaltopoulou T, Sergentanis TN, Panagiotakos DB, et al. Mediterranean diet, stroke, cognitive impairment, and depression: a meta-analysis[J]. Ann Neurol, 2013, 74(4): 580-591. DOI: 10.1002/ana.23944. [17] Mora S, Cook N, Buring JE, et al. Physical activity and reduced risk of cardiovascular events: potential mediating mechanisms[J]. Circulation, 2007, 116(19): 2110-2118. DOI: 10.1161/CIRCULATIONAHA.107.729939. [18] Wannamethee G, Shaper AG. Physical activity and stroke in British middle aged men[J]. BMJ, 1992, 304(6827): 597-601. DOI: 10.1136/bmj.304.6827.597. [19] Abraham G, Malik R, Yonova-Doing E, et al. Genomic risk score offers predictive performance comparable to clinical risk factors for ischaemic stroke[J]. Nat Commun, 2019, 10(1): 5819. DOI: 10.1038/s41467-019-13848-1. [20] Raum E, Rothenbacher D, Ziegler H, et al. Heavy physical activity: risk or protective factor for cardiovascular disease? A life course perspective[J]. Ann Epidemiol, 2007, 17(6): 417-424. DOI: 10.1016/j.annepidem.2006.12.008. [21] Kurth T, Gaziano JM, Rexrode KM, et al. Prospective study of body mass index and risk of stroke in apparently healthy women[J]. Circulation, 2005, 111(15): 1992-1998. DOI: 10.1161/01.CIR.0000161822.83163.B6. [22] Rutten-Jacobs LC, Larsson SC, Malik R, et al. Genetic risk, incident stroke, and the benefits of adhering to a healthy lifestyle: cohort study of 306 473 UK Biobank participants[J]. BMJ, 2018, 363: k4168. DOI: 10.1136/bmj.k4168. [23] 张海庆, 何美安, 张晓敏. 生活方式变化与新发脑卒中及其亚型的关联[J]. 中华疾病控制杂志, 2021, 25(3): 259-265. DOI: 10.16462/j.cnki.zhjbkz.2021.03.003.Zhang HQ, He MA, Zhang XM. Association of lifestyle change with incident stroke and its subtypes[J]. Chin J Dis Control Prev, 2021, 25(3): 259-265. DOI: 10.16462/j.cnki.zhjbkz.2021.03.003. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 606
- HTML全文浏览量: 182
- PDF下载量: 123
- 被引次数: 0