

Analysis on distribution and epidemic characteristics of common pathogens of pneumonia among hospitalized children, Suzhou, 2011-2018
-
摘要:
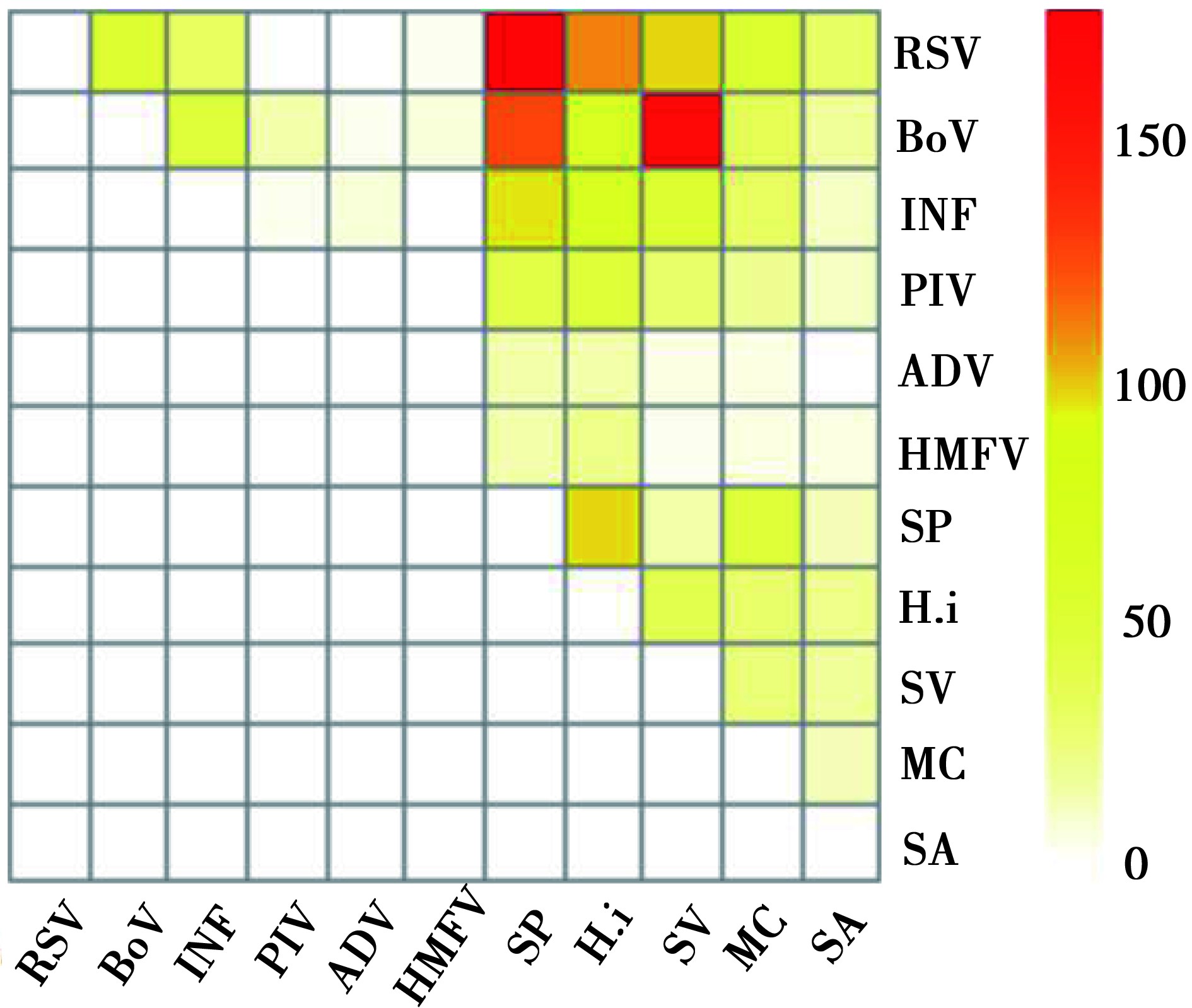
目的 了解苏州市住院儿童肺炎的病原分布特点及流行特征。 方法 以2011年4月-2018年3月入住苏州大学附属儿童医院呼吸科的临床肺炎住院儿童为对象, 采集鼻咽分泌物, 对儿童肺炎常见的细菌和病毒病原进行检测。 结果 4 765名临床肺炎病例中, 病原检出阳性3 602例(75.6%), 细菌检出阳性2 736例(57.4%), 阳性率最高的为肺炎链球菌(Streptococcus pneumoniae, SP)(20.3%), 其次为流感嗜血杆菌(Haemophilus influenzae, H.i)(15.5%); 病毒检出阳性2 101例(44.1%), 阳性率最高的为呼吸道合胞病毒(respiratory syncytial virus, RSV)(16.4%), 其次为博卡病毒(bocavirus, BoV)(13.6%)。细菌和病毒混合感染1 235例(25.9%), 最主要类型为呼吸道合胞病毒和肺炎链球菌、博卡病毒和草绿色链球菌(Streptococcus viride, SV)。 结论 SP、H.i、RSV、BoV是临床肺炎最主要的病原, 病原分布在月龄、季节上存在统计学差异, 细菌和病毒混合感染率较高。 Abstract:Objective To understand the distribution and epidemic characteristics of common pathogens of pneumonia among hospitalized children in Suzhou. Methods Nasopharyngeal secretions were collected from hospitalized children with clinical pneumonia admitted to the respiratory department of Children's Hospital Affiliated to Suzhou University from April 2011 to March 2018 to detect common viral and bacterial pathogens of children's pneumonia. Results The total positive rate of pathogens was 75.6% in the 4 765 clinical pneumonia cases. The positive rate of bacterial pathogens was 57.4%. Streptococcus pneumoniae(SP) was the highest, followed by Haemophilus influenzae(H.i); The positive rate of viral pathogens was 44.1%. Respiratory syncytial virus(RSV) was the highest, followed by Bocavirus(BoV). The mixed infection rate of bacteria and virus was 25.9%, and the most common types were RSV and SP, BoV and Streptococcus viride(SV). Conclusions SP, H.i, RSV and BoV are the main pathogens of clinical pneumonia in children. There are statistical differences in different age groups and seasons of hospitalized children's pneumonia in Suzhou. The mixed infection rate of bacteria and virus is high. -
Key words:
- Hospitalized children /
- Clinical pneumonia /
- Pathogenic distribution
-
表 1 研究对象与排除对象的基本特征分析[n (%)]
Table 1. Basic characteristics of research objects and exclusion objects [n (%)]
特征 纳入对象(n=4 765) 排除对象(n=1 062) χ2/Z值 P值 性别 1.79 1.181 男 2 941(61.7) 632(59.5) 女 1 824(38.3) 430(40.5) 年龄(月) -1.55 0.122 ≤6 1197(25.1) 265(25.0) 7~ 934(19.6) 172(16.2) 13~ 2 549(53.5) 605(57.0) > 60 85(1.8) 20(1.9) 季节 7.78 0.051 春季 1 287(27.0) 267(25.1) 夏季 995(20.9) 246(23.2) 秋季 1 075(22.6) 265(25.0) 冬季 1 408(29.5) 284(26.7)  下载: 导出CSV
下载: 导出CSV
表 2 儿童肺炎主要病原的月龄特点[n (%)]
Table 2. Age characteristics of main pathogens of pneumonia in children[n (%)]
≤6月龄 7~月龄 13~月龄 > 60月龄 χ2值 P值 (n=1 197) (n=934) (n=2 549) (n=85) 细菌性病原 81.79 < 0.001 SP 149(12.4) 204(21.8) 597(23.4) 16(18.8) 62.51 < 0.001 H.i 197(16.5) 180(19.3) 355(13.9) 5(5.9) 21.84 < 0.001 SV 159(13.3) 142(15.2) 331(13.0) 10(11.8) 31.17 0.366 MC 63(5.3) 60(6.4) 166(6.5) 0(0.0) 7.95 0.047 SA 131(10.9) 21(2.2) 38(1.5) 3(3.5) 197.21 < 0.001 E.coli 18(1.5) 5(0.5) 3(0.1) 0(0.0) - < 0.001a PA 9(0.8) 5(0.5) 9(0.4) 0(0.0) - 0.379a K.pn 9(0.8) 3(0.3) 1(0.0) 0(0.0) - 0.001a 病毒性病原 476(39.8) 447(47.9) 1 156(45.4) 22(25.9) 25.43 < 0.001 RSV 304(25.4) 178(19.1) 297(11.7) 1(1.2) 131.96 < 0.001 BoV 48(4.0) 139(14.9) 448(17.6) 12(14.1) 129.47 < 0.001 IFVA 39(3.3) 64(6.9) 191(7.5) 1(1.2) 29.56 < 0.001 IFVB 17(1.4) 29(3.1) 98(3.8) 4(4.7) 16.65 0.001 PIV 51(4.3) 57(6.1) 113(4.4) 1(1.2) 7.42 0.060 HMPV 29(2.4) 20(2.1) 45(1.8) 3(3.5) 2.84 0.418 ADV 5(0.4) 11(1.2) 61(2.4) 0(0.0) 23.02 < 0.001 注:a对E.coli、PA、K.pn的月龄分布特点分析采用确切概率法。
下载: 导出CSV
表 3 儿童肺炎主要病原的季节特点[n (%)]
Table 3. Seasonal characteristics of main pathogens of pneumonia in children[n (%)]
春季 夏季 秋季 冬季 χ2值 P值 (n=1 287) (n=995) (n=1 075) (n=1 408) 细菌性病原 43.67 < 0.001 SP 251(19.5) 167(16.8) 253(23.5) 295(21.0) 15.45 0.001 H.i 329(25.6) 118(11.9) 65(6.0) 225(16.0) 183.50 < 0.001 SV 135(10.5) 185(18.6) 221(20.6) 101(7.2) 126.42 < 0.001 MC 68(5.3) 55(5.5) 86(8.0) 80(5.7) 9.31 0.025 SA 58(4.5) 42(4.2) 41(3.8) 52(3.7) 1.38 0.710 E.coli 7(0.5) 6(0.6) 7(0.7) 6(0.4) 65.20 0.885 PA 3(0.2) 6(0.6) 11(1.0) 3(0.2) 10.63 0.014 K.pn 0(0.0) 6(0.6) 3(0.3) 4(0.3) - 0.030a 病毒性病原 505(39.2) 438(44.0) 484(45.0) 674(47.9) 20.83 < 0.001 RSV 147(11.4) 20(2.0) 236(22.0) 377(26.8) 162.58 < 0.001 细菌性病原 791(61.5) 561(56.4) 668(62.1) 716(50.9) 43.67 < 0.001 SP 251(19.5) 167(16.8) 253(23.5) 295(21.0) 15.45 0.001 H.i 329(25.6) 118(11.9) 65(6.0) 225(16.0) 183.50 < 0.001 SV 135(10.5) 185(18.6) 221(20.6) 101(7.2) 126.42 < 0.001 注:a对K.pn的季节分布特点分析采用确切概率法。
下载: 导出CSV
表 4 儿童肺炎病原混合感染情况[n (%)]
Table 4. Mixed infection of pneumonia in children[n (%)]
n 合并其他细菌感染 合并其他病毒感染 细菌-病毒混合感染 RSV 780 - 86(11.0) 451(57.8) BoV 647 - 121(18.7) 412(63.7) INF 443 - 91(20.5) 253(57.1) PIV 222 - 26(11.7) 133(59.9) ADV 77 - 6(7.8) 37(48.1) HMPV 97 - 12(12.4) 40(41.2) SP 851 167(19.6) - 430(50.5) H.i 737 182(24.7) - 295(40.0) SV 642 91(14.2) - 324(50.5) MC 289 111(38.4) - 140(48.4) SA 193 61(31.6) - 66(34.2)
下载: 导出CSV
-
[1] Cevey-Macherel M, Galetto-Lacour A, Gervaix A, et al. Etiology of community-acquired pneumonia in hospitalized children based on WHO clinical guidelines[J]. Eur J Pediatr, 2009, 168(12): 1429-1436. DOI: 10.1007/s00431-009-0943-y. [2] 中华医学会儿科学分会呼吸学组, 编辑委员会中华儿科杂志.儿童社区获得性肺炎管理指南(2013修订)(上)[J].中华儿科杂志, 2013, 51(10): 745-752. DOI: 10.3760/cma.j.issn.0578-1310.2013.10.006.Respiratory group, society of pediatrics, Chinese Society of Pediatrics, editorial board, Chinese Journal of Pediatrics. Guidelines for the management of community-acquired pneumonia in children(revised in 2013)(I)[J]. Chin J Pediatr, 2013, 51(10): 745-752. DOI: 10.3760/cma.j.issn.0578-1310.2013.10.006. [3] 彭懿, 舒畅, 符州, 等.儿童社区获得性肺炎1613例病原学特点分析[J].中国当代儿科杂志, 2015(11): 1193-1199. DOI: 10.7499/j.issn.1008-8830.2015.11.009.Peng Y, Shu C, Fu Z, et al. Pathogen detection of 1 613 cases of hospitalized children with community acquired pneumonia[J]. Chin J Contemp Pediatr, 2015, 17(11): 1193-1199. DOI: 10.7499/j.issn.1008-8830.2015.11.009. [4] 冯录召, 赖圣杰, 李夫, 等. 2009-2012年我国6省(市)5岁以下儿童住院肺炎病例的病毒病原学分析[J].中华流行病学杂志, 2014(6): 646-649. DOI: 10.3760/cma.j.issn.0254-6450.2014.06.007.Feng LZ, Lai SJ, Li F, et al. Viral etiologies of hospitalized pneumonia patients aged less than five years in six provinces, 2009-2012[J]. Chin J Epidemiol, 2014(6): 646-649. DOI: 10.3760/cma.j.issn.0254-6450.2014.06.007. [5] De-Schutter I, De-Wachter E, Crokaert F, et al. Microbiology of bronchoalveolar lavage fluid in children with acute nonresponding or recurrent community-acquired pneumonia: identification of nontypeable haemophilus influenzae as a major pathogen[J]. Clin Infect Dis, 2011, 52(12): 1437-1444. DOI: 10.1093/cid/cir235. [6] Ferone EA, Berezin EN, Durigon GS, et al. Clinical and epidemiological aspects related to the detection of adenovirus or respiratory syncytial virus in infants hospitalized for acute lower respiratory tract infection[J]. Jornal de Pediatria, 2014, 90(1): 42-49. DOI: 10.1016/j.jped.2013.05.005. [7] 黄志英, 程宝金, 林红, 等. 80例住院患儿腺病毒呼吸道感染的流行病学特点和临床特征分析[J].病毒学报, 2014, 30(4): 408-411. DOI: 10.13242/j.cnki.bingduxuebao.002524.Huang ZY, Cheng BJ, Lin H, et al. Epidemiological and clinical characteristics of adenovirus respiratory tract infections in 80 hospitalized children[J]. Chin J Virol, 2014, 30(4): 408-411. DOI: 10.13242/j.cnki.bingduxuebao.002524. [8] 冯英, 罗征秀, 符州, 等.重庆地区婴幼儿社区获得性肺炎病原学分析[J].儿科药学杂志, 2011, 17(5): 39-42. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=ekyx201105015Feng Y, Luo ZX, Fu Z, et al. Etiology of children with community acquired pneumonia in chongqing area[J]. J Pediatr Pharm, 2011, 17(5): 39-42. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=ekyx201105015 [9] 罗蓉, 符州, 黄英, 等. 99例儿童腺病毒肺炎临床特征分析[J].重庆医学, 2014(30): 3997-3998, 4001. DOI: 10.3969/j.issn.1671-8348.2014.30.005.Luo R, Fu Z, Huang Y, et al. Clinical characteristic analysis of 99 adenovirus pneumonia cases in children[J]. Chongqing Med, 2014(30): 3997-3998, 4001. DOI: 10.3969/j.issn.1671-8348.2014.30.005. [10] 陈倩, 施圣云, 胡正, 等.南京地区急性呼吸道感染儿童支原体、衣原体和常见呼吸道病毒病原学分析[J].中国当代儿科杂志, 2010, 12(6): 450-454. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=zgddekzz201006010Chen Q, Shi SY, Hu Z, et al. Pathogenic analysis of mycoplasma, chlamydia and common respiratory viruses in children with acute respiratory infections in Nanjing[J]. Chin J Contemp Pediatr, 2010, 12(6): 450-454. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=zgddekzz201006010 [11] Nascimento-Carvalho CM, Cardoso MA, Barral A, et al. Seasonal patterns of viral and bacterial infections among children hospitalized with community-acquired pneumonia in a tropical region[J]. Scand J Infect Dis, 2010, 42(11-12): 839-844. DOI: 10.3109/00365548.2010.498020. [12] 张国英, 夏学红, 吕连峥. 503例儿童急性呼吸道感染常见病毒的检测结果分析[J].中国微生态学杂志, 2014, 26(10): 1206-1208. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=zgwstxzz201410027Zhang GY, Xia XH, Lu LZ. Detection results of common viruses in 503 children with acute respiratory infections[J]. Chin J Microecol, 2014, 26(10): 1206-1208. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=zgwstxzz201410027 [13] Prel JD, Puppe W, Grondahl B, et al. Are meteorological parameters associated with acute respiratory tract infections?[J]. Clin Infect Dis, 2009, 49(6): 861-868. DOI: 10.1086/605435. [14] Hament J, Aerts PC, Fleer A, et al. Enhanced adherence of streptococcus pneumoniae to human epithelial cells infected with respiratory syncytial virus[J]. Pediatr Res, 2004, 55(6): 972-978. DOI: 10.1203/01.PDR.0000127431.11750.D9. [15] Vasanthi A, Rodriguez CA, DeVincenzo JP, et al. Respiratory viruses augment the adhesion of bacterial pathogens to respiratory epithelium in a viral species-and cell type-dependent manner[J]. J Virol, 2006, 80. DOI: 10.1128/JVI.80.4.1629. [16] Papadopoulos NG, Moustaki M, Tsolia M, et al. Association of rhinovirus infection with increased disease severity in acute bronchiolitis[J]. Am J Respir Crit Care Med, 2002, 165(9): 1285-1289. DOI: 10.1164/rccm.200112-118BC. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 161
- HTML全文浏览量: 155
- PDF下载量: 35
- 被引次数: 0