

Progress towards the UNAIDS 90-90-90 targets and factors associated with achieving these targets
-
摘要:
目的 分析南京市2018年艾滋病防治策略“三个90%”目标的进展情况及其实现的影响因素。 方法 从艾滋病防治综合信息系统中获取南京市现存活的人类免疫缺陷病毒(human immunodeficiency virus, HIV)感染者/艾滋病(acquired immune deficiency syndrome, AIDS)患者检测发现、抗病毒治疗(antiviral therapy, ART)和病毒载量(viral load, VL)相关信息,分析“三个90%”进展情况,采用多因素Logistic回归分析模型分析影响因素。 结果 2018年南京市“三个90%”目标分别达到74.0%、88.5%和96.7%。经同性传播的HIV/AIDS检测发现率较低(χ2 =86.15, P < 0.001)。注射吸毒传播(aOR=0.263,95% CI:0.156~0.442,P < 0.001)、 < 25岁年龄组(aOR=0.697,95% CI:0.540~0.899,P=0.005)以及监管场所发现(aOR= 0.353,95% CI:0.193~0.646,P=0.001)的HIV/AIDS治疗覆盖率较低;而同性传播(aOR=1.840,95% CI:1.390~2.434,P < 0.001)、35~44岁年龄组(aOR=1.826,95% CI:1.260~2.645,P=0.001)、汉族(aOR=1.797,95% CI:1.038~3.109,P=0.036)、大专及以上文化程度(aOR=1.652,95% CI:1.005~2.717,P=0.048)、已婚有配偶(aOR=1.466,95% CI:1.051~2.046,P=0.024)的HIV/AIDS治疗覆盖率较高。 结论 南京市朝着2020年实现“三个90%”的防治目标迅速迈进,但仍有一定的挑战,需要继续扩大HIV检测发现,加强吸毒人群、低龄和老年人等重点人群治疗关怀服务。 Abstract:Objective To analyze the current status towards the UNAIDS 90-90-90 targets and factors associated with achieving these targets in Nanjing. Methods Data from the Chinese HIV/AIDS Comprehensive Response Information Management System regarding testing, ART and VL in Nanjing were collected. Multivariate Logistic regression analysis was performed to analyze the associated factors with achieving the 90-90-90 targets. Results The progress towards the 90-90-90 UNAIDS targets was at 74.0%, 88.5%, and 96.7% in Nanjing by 2018. HIV/AIDS infected by homosexual contact were less likely to be diagnosed (χ2 =86.15, P < 0.001) People living with HIV (PLWH) infected through injecting drug use (aOR=0.263, 95% CI:0.156-0.442, P < 0.001), aged < 25 years (aOR=0.697, 95% CI:0.540-0.899, P=0.005) and identified from custodial institutions (aOR=0.353, 95% CI:0.193-0.646, P=0.001) were less likely to engage on ART. PLWH infected through homosexual contact (aOR=1.840, 95% CI:1.390-2.434, P < 0.001), aged 35-44 years (aOR=1.826, 95% CI:1.260-2.645, P=0.001), ethnic group of Han (aOR=1.797, 95% CI:1.038-3.109, P=0.036), of college degree or above (aOR=1.652, 95% CI:1.005-2.717, P=0.048) and married (aOR=1.466, 95% CI:1.051-2.046, P=0.024) were more likely to engage on ART. Conclusions Nanjing is rapidly moving towards achieving the UN targets. However, some challenges still exist. We need to continue to expand HIV testing and strengthen the treatment and care services for drug users, young people and the elderly. -
Key words:
- AIDS /
- Prevention and treatment strategies /
- 90-90-90 targets /
- Associated factors
-
抗病毒治疗的广泛使用可以有效减少人类免疫缺陷病毒(human immunodeficiency virus, HIV)传播,在全球控制艾滋病流行战略中可发挥重要作用[1]。早期开始抗病毒治疗不仅降低了HIV/艾滋病(acquired immune deficiency syndrome, AIDS)的死亡率,而且降低了HIV的发病率,从而产生了“治疗即预防”的概念[2-3]。美国一项随机对照试验研究[4]表明,在一方是HIV阳性一方是HIV阴性的单阳夫妻中实施早期抗病毒治疗可以降低96%的HIV新发感染。2014年联合国艾滋病毒/艾滋病联合规划署提出了90-90-90的防治目标[5],即到2020年,至少90%的存活感染者知晓自身的感染状况,至少90%已经确诊的感染者接受抗病毒治疗,90%接受抗病毒治疗的感染者病毒得到抑制。中国也将“三个90%”目标列为《中国遏制与防治艾滋病“十三五”行动计划》目标。为实现该防治策略,从而有效控制南京市艾滋病流行,本次研究旨在评估南京市2018年90-90-90防治目标的进展状况,并分析接受抗病毒治疗和病毒载量(viral load, VL)达到抑制的相关因素,确定较难实现目标的高风险人群亚组,为进一步推进“三个90%”目标提供科学依据。
1. 对象与方法
1.1 研究对象
截至2018年12月31日仍存活的所有现住址为南京市并且年龄≥18个月的HIV/AIDS感染者,不包括在本年转化为AIDS的既往HIV感染者。
1.2 研究方法
1.2.1 数据收集
收集截至2018年12月31日,南京市估计现存活HIV/AIDS数、检测发现HIV/AIDS数、接受抗病毒治疗及病毒载量得到抑制的HIV/AIDS数,计算检测发现率、抗病毒治疗覆盖率及病毒抑制率,分析影响检测发现、接受抗病毒治疗及病毒抑制的影响因素。
1.2.2 资料来源
(1)现存活HIV/AIDS数来源于南京市2018年艾滋病疫情估计分析;(2)现存活HIV/AIDS报告病例数及治疗相关信息来源于艾滋病防治基本信息系统,包括社会人口学特征、开始治疗时CD4+T淋巴细胞(简称“CD4”)计数、抗病毒治疗情况及病毒载量检测值等。
1.2.3 相关指标及定义
(1) 现存活HIV/AIDS估计数:采用UNAIDS推荐的Workbook法估计南京市2018年现存活HIV/AIDS数;(2)检测发现率:分子为艾滋病防治基本信息系统中已终审的HIV临床诊断病例和确诊病例,分母为现存活HIV/AIDS估计数;(3)抗病毒治疗覆盖率:分子为接受抗病治疗且2018年12月31日前仍在治或者转诊的HIV/AIDS,分母为艾滋病防治基本信息系统中已终审的HIV临床诊断病例和确诊病例;(4)病毒载量抑制率:世界卫生组织(world health organization,WHO)将病毒载量 < 1 000拷贝/ml定义为达到抑制,治疗满半年的HIV/AIDS才能进行免费病毒载量检测,本研究将病毒载量是否抑制的观察终止时间延长至2019年12月31日,病毒载量抑制率分子为2019年12月31前最后1次VL < 1 000拷贝/ml的在治HIV/AIDS人数,分母为2018年12月31日前接受抗病毒治疗且仍在治的HIV/AIDS人数。
1.3 统计学方法
应用SPSS 20.0软件进行统计分析。不同性别和传播途径的检测发现率的比较采用χ2检验。接受抗病毒治疗的影响因素分析采用多因素Logistic回归分析模型,以是否接受抗病毒治疗为因变量(0=未接受,1=接受),自变量包括性别、感染途径、发现时年龄、民族、文化程度、婚姻状况及样本来源。病毒载量抑制的影响因素分析采用多因素Logistic回归分析模型,以病毒载量是否抑制(0=否,1=是),自变量包括性别、感染途径、发现时年龄、民族、文化程度、婚姻状况、样本来源以及开始抗病毒治疗时CD计数。检验水准α=0.05。
2. 结果
2.1 检测发现情况
应用Workbook法估计,截至2018年12月31日,南京市现存活HIV/AIDS估计数为5 299(3 566~7 032)例,检测发现数为3 922例,检测发现率为74.0%,经同性传播的病例检测发现率较低(χ2 =86.148,P < 0.001)。见表 1。
表 1 南京市2018年检测发现率进展情况及相关因素分析Table 1. Progress towards detection rate and related factors in Nanjing City by 2018变量 估计数 报告数(%) χ2值 P值 性别 1.403 0.236 女 376 288(76.6) 男 4 923 3 634(73.8) 感染途径 86.148 < 0.001 异性传播 1 202 993(82.6) 同性传播 3 978 2 820(70.9) 注射吸毒 104 94(90.4) 血液/母婴传播 15 15(100.0) 2.2 接受抗病毒治疗情况
抗病毒治疗覆盖率为88.5%(3 470/3 922)。多因素Logistic回归分析模型分析结果显示,注射吸毒传播、 < 25岁年龄组以及监管场所发现的HIV/AIDS治疗覆盖率较低;而同性传播、35~岁年龄组、汉族、大专及以上文化程度、已婚有配偶的HIV/AIDS治疗覆盖率较高。见表 2。
表 2 南京市2018年抗病毒治疗覆盖率和病毒抑制率进展情况及相关因素分析Table 2. Progress and related factors of antiviral therapy coverage rate and viral load suppression rate in Nanjing City by 2018变量 现存活数 抗病毒治疗 病毒载量抑制 例数[n(%)] aOR(95% CI)值 P值 例数[n(%)] aOR(95% CI)值 P值 性别 女 288 240(83.3) 1.000 233(97.5) 1.000 男 3 634 3 230(88.9) 0.997(0.669~1.484) 0.986 3 108(96.7) 0.502(0.197~1.279) 0.148 感染途径 异性传播 993 857(86.3) 1.000 831(97.1) 1.000 同性传播 2 820 2 544(90.2) 1.840(1.390~2.434) < 0.001 2 457(96.9) 1.019(0.583~1.782) 0.946 注射吸毒 94 54(57.4) 0.263(0.156~0.442) < 0.001 40(80.0) 0.110(0.041~0.293) 0.000 血液/母婴传播 15 15(100.0) 13(100.0) 0.999 报告年龄(岁) < 25 985 841(85.4) 0.697(0.540~0.899) 0.005 796(95.1) 0.346(0.202~0.591) < 0.001 25~ 1 363 1 206(88.5) 1.000 0.001 1 177(98.1) 1.000 35~ 708 648(91.5) 1.826(1.260~2.645) 0.001 623(97.0) 0.935(0.448~1.951) 0.858 45~ 562 511(90.9) 1.439(0.958~2.162) 0.079 497(97.3) 0.883(0.390~2.002) 0.766 ≥55 304 264(86.8) 0.929(0.593~1.455) 0.748 248(93.9) 0.355(0.155~0.810) 0.014 民族 少数民族 90 72(80.0) 1.000 70(98.6) 1.000 汉族 3 832 3 398(88.7) 1.797(1.038~3.109) 0.036 3 271(96.7) 0.478(0.065~3.517) 0.469 文化程度 文盲/小学 196 164(83.7) 1.000 151(93.8) 1.000 初中/高中 1 662 1 459(87.8) 1.308(0.829~2.065) 0.249 1 398(96.3) 1.997(0.934~4.270) 0.075 大专及以上 2 064 1 847(89.5) 1.652(1.005~2.717) 0.048 1 792(97.3) 3.020(1.293~7.055) 0.011 婚姻状况 未婚 2 236 1 948(87.1) 1.000 1 864(96.4) 1.000 已婚有配偶 1 149 1 042(90.7) 1.466(1.051~2.046) 0.024 1 014(97.4) 1.545(0.805~2.967) 0.191 离异或丧偶 537 480(89.4) 1.203(0.811~1.785) 0.359 463(96.5) 1.164(0.564~2.400) 0.682 样本来源 医疗机构 1 420 1 275(89.8) 1.000 1 228(96.5) 1.000 检测咨询 1 809 1 602(88.6) 0.813(0.636~1.039) 0.098 1 544(96.8) 0.971(0.620~1.521) 0.898 监管场所 70 43(61.4) 0.353(0.193~0.646) 0.001 34(89.5) 0.959(0.254~3.620) 0.951 专题调查 285 259(90.9) 0.966(0.609~1.530) 0.882 250(97.3) 1.168(0.504~2.708) 0.718 其他 338 291(86.1) 0.793(0.552~1.139) 0.210 285(97.9) 1.709(0.705~4.145) 0.236 开始抗病毒治疗时CD4计数(个/μl) < 200 1 160 1 110(95.7) 1.000 201~ 1 114 1 081(97.0) 1.561(0.976~2.496) 0.063 ≥351 1 180 1 150(97.5) 1.880(1.149~3.078) 0.012 2.3 病毒载量抑制情况
接受抗病毒治疗的3 470例HIV/AIDS中,16人在外地定点治疗机构治疗,病毒载量抑制情况缺失,在治HIV/AIDS的病毒抑制率为96.7%(3 341/3 454)。多因素Logistic回归分析模型分析结果显示,注射吸毒传播、 < 25岁年龄组和≥55岁年龄组的在治HIV/AIDS病毒抑制率较低;大专及以上文化程度和开始治疗时CD4计数≥351个/μl的病毒抑制率较高。见表 2。
2.4 不同传播途径的“三个90%”进展情况
2018年底,南京市“三个90%”目标已达到74.0%-88.5%-96.7%,同性传播、异性传播和注射吸毒传播的HIV/AIDS“三个90%”目标分别达到70.9%-90.2%-96.9%、82.6%-86.3%-97.1%和90.4%-57.4%-80.0%。见图 1。
 图 1 不同传播途径的HIV/AIDS三个90%的进展情况Figure 1. Progress towards the UNAIDS 90-90-90 targets by routes of transmission
图 1 不同传播途径的HIV/AIDS三个90%的进展情况Figure 1. Progress towards the UNAIDS 90-90-90 targets by routes of transmission3. 讨论
南京市2018年底检测发现率74.0%,治疗覆盖率为88.5%,病毒抑制率为96.7%,2015年底中国、山东省和重庆市[6-7]这三项目标分别达到68%-67%-91%、61.2%-74.4%-81.8%和56.8%-68.0%-90.9%,南京市2013-2015年作为男男性行为人群HIV扩大检测扩大治疗的试点城市之一,2016-2018年通过政府购买社会组织服务在高危人群中开展干预工作和动员HIV检测工作,2014-2018年创建艾滋病第三轮综合防治示范区时重点推进性病门诊就诊者扩大HIV检测和32家医疗卫生机构医务人员主动提供HIV检测服务(provider initiated testing and counseling, PITC)等创新工作,目前南京市正朝着目标迅速迈进,但检测发现率仍有一定的差距,而第一个90%的实现是实现治疗覆盖率和病毒抑制率两个90%的基础。
2018年底南京市有26%的存活HIV感染者未能被诊断,因此,进一步扩大HIV检测覆盖率和提高检测咨询服务质量尤为重要,扩大检测不仅需要开展针对性宣传来提高主动检测意识,同时需要进一步完善HIV检测网络建设,将自愿咨询检测、PITC、高危人群社区组织动员检测、社区卫生服务中心快检点以及自我检测等多种体系相结合,从而发现更多的HIV感染者。本次研究发现同性传播途径的感染者检测发现率较低。研究表明担心受到歧视、担心检测阳性、缺乏转介机制、不知道哪里可以做免费HIV检测等因素会影响男男性行为者主动检测[8]。检测意愿是HIV检测行为的重要预测因素,需要在MSM社区进一步倡导检测的意义和宣传PITC相关信息,提高其检测意愿从而促进其参加HIV检测。南京市高达四分之三的MSM通过互联网/交友软件寻找性伴侣[9],提示可以通过社交软件对MSM进行线上艾滋病宣传干预工作,在社交软件定期推送宣传资料和PITC等信息,引导有检测需求的MSM前往HIV自愿咨询检测门诊、医院或者社区组织及时进行检测。
2016年6月,国家卫生计生委调整抗病毒治疗的标准,为所有愿意接受抗病毒治疗的病人提供免费抗病毒治疗,为实现第二个90%目标提供了政策保障。研究发现经注射吸毒传播的和监管场所发现的感染者治疗覆盖率,由于注射吸毒人群主要是羁押场所发现,其治疗覆盖率低可能与他们对自身健康的重视度低有关,而且该人群的随访管理和转介治疗难度较大,目前南京市已经基本建立了HIV罪犯集中关押场所,因此,需要进一步联合公安部门保障狱内治疗工作的落实。多项研究[10-11]发现注射吸毒传播是停药和终止治疗的危险因素,提示需关注已治疗罪犯的刑满释放后续随访,监狱提供一到两个月量的药品、书面的治疗方案、户籍所在定点医院电话等,以保证其出狱后继续服药。本研究发现年轻感染者治疗覆盖率较低,可能与自认为身体好没有出现临床症状不愿意启动抗病治疗有关,同时有研究[10]发现年龄小的感染者容易脱失和终止抗病毒治疗,因此今后需要关注低年龄组病例的治疗转介咨询工作。
陈洋等[12]研究表明年龄是病毒抑制的危险因素,低年龄组病毒抑制失败率较高,本研究发现不仅年轻人病毒抑制率较低,老年患者的病毒抑制成功率也较低,可能是由于老年人开始治疗时基线免疫水平较低,容易出现机会性感染,体内HIV病毒复制较难得到抑制,免疫系统重建较难实现。本研究显示注射吸毒传播的病毒抑制率较低,和国外研究[11]基本一致。由于抗病毒治疗需要长期坚持服药,服药依从性对治疗效果尤为重要,研究[13]发现影响抗病毒治疗依从性的主要因素包括文化程度、婚姻状况及传播途径等,本次研究发现不同传播途径和文化程度的病毒抑制率的差异可能与治疗依从性有关。开始治疗时CD4水平高的患者病毒抑制成功率较高,有研究表明开始治疗时CD4水平越高耐药发生的风险越低[14],这主要由于CD4水平与患者免疫有关,基线CD4水平较高的患者免疫功能尚可,体内病毒抑制的效果较好,这也提示早期HIV抗病毒治疗才能更好地实现成功治疗这一目标。
总之,南京实现“三个90%”虽然有一定的挑战性,但是瑞典、博茨瓦纳和丹麦等[15-16]国家成功的经验表明这一目标是可以实现的。南京市需要继续扩大HIV检测,加强吸毒人群和低年龄组的病例咨询和治疗转介工作;关注吸毒人群、低龄和55岁以上老年人、文化程度较低的患者以及基线CD4水平较低的患者的病毒载量和依从性教育,有针对性地优化防控重点,尽早实现“三个90%”防治目标。
-
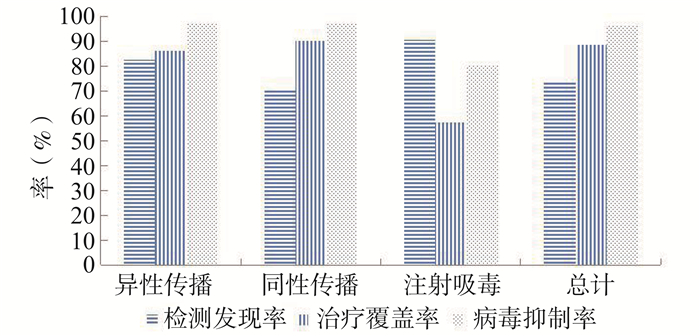
图 1 不同传播途径的HIV/AIDS三个90%的进展情况
Figure 1. Progress towards the UNAIDS 90-90-90 targets by routes of transmission
表 1 南京市2018年检测发现率进展情况及相关因素分析
Table 1. Progress towards detection rate and related factors in Nanjing City by 2018
变量 估计数 报告数(%) χ2值 P值 性别 1.403 0.236 女 376 288(76.6) 男 4 923 3 634(73.8) 感染途径 86.148 < 0.001 异性传播 1 202 993(82.6) 同性传播 3 978 2 820(70.9) 注射吸毒 104 94(90.4) 血液/母婴传播 15 15(100.0)  下载: 导出CSV
下载: 导出CSV
表 2 南京市2018年抗病毒治疗覆盖率和病毒抑制率进展情况及相关因素分析
Table 2. Progress and related factors of antiviral therapy coverage rate and viral load suppression rate in Nanjing City by 2018
变量 现存活数 抗病毒治疗 病毒载量抑制 例数[n(%)] aOR(95% CI)值 P值 例数[n(%)] aOR(95% CI)值 P值 性别 女 288 240(83.3) 1.000 233(97.5) 1.000 男 3 634 3 230(88.9) 0.997(0.669~1.484) 0.986 3 108(96.7) 0.502(0.197~1.279) 0.148 感染途径 异性传播 993 857(86.3) 1.000 831(97.1) 1.000 同性传播 2 820 2 544(90.2) 1.840(1.390~2.434) < 0.001 2 457(96.9) 1.019(0.583~1.782) 0.946 注射吸毒 94 54(57.4) 0.263(0.156~0.442) < 0.001 40(80.0) 0.110(0.041~0.293) 0.000 血液/母婴传播 15 15(100.0) 13(100.0) 0.999 报告年龄(岁) < 25 985 841(85.4) 0.697(0.540~0.899) 0.005 796(95.1) 0.346(0.202~0.591) < 0.001 25~ 1 363 1 206(88.5) 1.000 0.001 1 177(98.1) 1.000 35~ 708 648(91.5) 1.826(1.260~2.645) 0.001 623(97.0) 0.935(0.448~1.951) 0.858 45~ 562 511(90.9) 1.439(0.958~2.162) 0.079 497(97.3) 0.883(0.390~2.002) 0.766 ≥55 304 264(86.8) 0.929(0.593~1.455) 0.748 248(93.9) 0.355(0.155~0.810) 0.014 民族 少数民族 90 72(80.0) 1.000 70(98.6) 1.000 汉族 3 832 3 398(88.7) 1.797(1.038~3.109) 0.036 3 271(96.7) 0.478(0.065~3.517) 0.469 文化程度 文盲/小学 196 164(83.7) 1.000 151(93.8) 1.000 初中/高中 1 662 1 459(87.8) 1.308(0.829~2.065) 0.249 1 398(96.3) 1.997(0.934~4.270) 0.075 大专及以上 2 064 1 847(89.5) 1.652(1.005~2.717) 0.048 1 792(97.3) 3.020(1.293~7.055) 0.011 婚姻状况 未婚 2 236 1 948(87.1) 1.000 1 864(96.4) 1.000 已婚有配偶 1 149 1 042(90.7) 1.466(1.051~2.046) 0.024 1 014(97.4) 1.545(0.805~2.967) 0.191 离异或丧偶 537 480(89.4) 1.203(0.811~1.785) 0.359 463(96.5) 1.164(0.564~2.400) 0.682 样本来源 医疗机构 1 420 1 275(89.8) 1.000 1 228(96.5) 1.000 检测咨询 1 809 1 602(88.6) 0.813(0.636~1.039) 0.098 1 544(96.8) 0.971(0.620~1.521) 0.898 监管场所 70 43(61.4) 0.353(0.193~0.646) 0.001 34(89.5) 0.959(0.254~3.620) 0.951 专题调查 285 259(90.9) 0.966(0.609~1.530) 0.882 250(97.3) 1.168(0.504~2.708) 0.718 其他 338 291(86.1) 0.793(0.552~1.139) 0.210 285(97.9) 1.709(0.705~4.145) 0.236 开始抗病毒治疗时CD4计数(个/μl) < 200 1 160 1 110(95.7) 1.000 201~ 1 114 1 081(97.0) 1.561(0.976~2.496) 0.063 ≥351 1 180 1 150(97.5) 1.880(1.149~3.078) 0.012
下载: 导出CSV
-
[1] Karim SS, Karim QA. Antiretroviral prophylaxis: a defining moment in HIV control[J]. Lancet, 2011, 378(9809):e23-e25. DOI: 10.1016/S0140-6736(11)61136-7. [2] Mayer K, Gazzard B, Zuniga JM, et al. Controlling the HIV epidemic with antiretrovirals: IAPAC consensusstatement on treatment as prevention and preexposure prophylaxis[J]. J IntAssocProvid AIDS Care, 2013, 12(3):208-216. DOI: 10.1177/2325957413475839. [3] Cohen MS, Gay CL. Treatment to prevent transmission of HIV-1[J]. Clin Infect Dis, 2010, 50 Suppl 3(3):S85-S95. DOI: 10.1086/651478. [4] Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy[J]. N Engl MED, 2011, 365(6):493-505. DOI: 10.1056/NEJMoa1105243. [5] The Joint United Nations Programme on HIV and AIDS (UNAIDS). 90-90-90- An ambitious treatment target to help end the AIDS epidemic[EB/OL]. (2017-01-01)[2020-09-30]. https://www.unaids.org/en/resources/documents/2017/90-90-90. [6] 吴尊友.我国实现艾滋病防治策略三个90%的进展与挑战[J].中华疾病控制杂志, 2016, 20(12):1187-1189. DOI: 10.16462/j.cnki.zhjbkz.2016.12.001.Wu ZY. The progress and challenges of promoting HIV/AIDS 90-90-90 Strategies in China[J]. Chin J Dis Control Prev, 2016, 20(12):1187-1189. DOI: 10.16462/j.cnki.zhjbkz.2016.12.001. [7] 张娜, 黄涛, 杨兴光, 等.山东省2015年艾滋病防治策略"三个90%"目标进展状况分析[J].中华流行病学杂志, 2017, 38(10):1367-1371. DOI: 10.3760/cma.j.issn.0254-6450.2017.10.014.Zhang N, Huang T, Yang XG, et al. A cross-sectional study on HIV/AIDS "90-90-90" treatment target in Shandong Province, 2015[J]. Chin J Epidemiol, 2017, 38(10):1367-1371. DOI: 10.3760/cma.j.issn.0254-6450.2017.10.014. [8] Liu Y, Sun X, Qian HZ, et al. Qualitative assessment of barriers and facilitators of access to HIV testing among men who have sex with men in China[J]. AIDS Patient Care STDS, 2015, 29(9):481-489. DOI: 10.1089/apc.2015.0083. [9] 徐园园, 朱正平, 吴苏姝, 等.南京市男男性行为者新型毒品使用情况及相关因素[J].中华疾病控制杂志, 2019, 23(12):1476-1481. DOI: 10.16462/j.cnki.zhjbkz.2019.12.009.Xu YY, Zhu ZP, Wu SS, et al. Status and associated factors of recreational drug use among man who have sex with man in Nanjing[J]. Chin J Dis Control Prev, 2019, 23(12):1476-1481. DOI: 10.16462/j.cnki.zhjbkz.2019.12.009. [10] 李萌, 魏洪霞, 步凯, 等.南京和运城市HIV感染者及艾滋病患者终止抗病毒治疗情况及其影响因素[J].中华流行病学杂志, 2015, 36(10):1113-1118. DOI: 10.3760/cma.j.issn.0254-6450.2015.10.017.Li M, Wei HX, Bu K, et al. Drop out of antiretroviral therapy in people living with AIDS/HIV and related factors in Nanjing and Yuncheng[J]. Chin J Epidemiol, 2015, 36(10):1113-1118. DOI:10.3760/cma.j.issn. 0254-6450.2015.10.017. [11] Laut KG, Shepherd L, Gottfredsson M, et al. Variation in antiretroviral treatment coverage and virological suppression among three HIV key populations[J]. AIDS, 2018, 32(18):2807-2819. DOI: 10.1097/QAD.0000000000002035. [12] 陈洋, 申莉梅, 李豫, 等.贵州省艾滋病病人退出抗病毒治疗的情况及其影响因素分析[J].中国艾滋病性病, 2017, 23(5):397-401. DOI: 10.13419/j.cnki.aids.2017.05.08.Chen Y, Shen LM, Li Y, et al. Impact factors of withdramal from antiretrovial therapy among HIV/AIDS patients in Guizhou province[J]. China J AIDS STD, 2017, 23(5):397-401. DOI: 10.13419/j.cnki.aids.2017.05.08. [13] 丁昌棉, 杨银梅, 王威, 等.武汉市PLWHA抗病毒治疗服药依从性及相关因素[J].中华疾病控制杂志, 2018, 22(12): 1234-1237. DOI: 10.16462/j.cnki.zhjbkz.2018.12.008.Ding CM, YM, Wang W, et al. Study on adherence to antiretroviral therapy and its associated factors among people living with HIV/AIDS in Wuhan City[J]. Chin J Dis Control Prev, 2018, 22(12): 1234-1237. DOI: 10.16462/j.cnki.zhjbkz.2018.12.008. [14] 周莹, 卢静, 张之, 等.江苏省艾滋病一线药物抗病毒治疗失败病人的耐药特征及影响因素分析[J].中华疾病控制杂志, 2017, 21(12):1191-1194. DOI: 10.16462/j.cnki.zhjbkz.2017.12.002Zhou Y, Lu J, Zhang Z, et al. Risk factors associated with HIV drug resistance among ART virological failure patients taking first-line antiviral treatment from Jiangsu Province[J]. Chin J Dis Control Prev, 2017, 21(12):1191-1194. DOI: 10.16462/j.cnki.zhjbkz.2017.12.002. [15] Joint United Nations Programme on HIV/AIDS (UNAIDS). Ending HIV progress towards the 90-90-90 targets[EB/OL].(2017-01-01)[2020-09-30].https://www.unaids.org/en/resources/documents/2017/20170720_Global_AIDS_update_2017. [16] GisslénM, Svedhem V, Lindborg L, et al. Sweden, the first country to achieve the Joint United Nations Programme on HIV/AIDS (UNAIDS)/World Health Organization (WHO) 90-90-90 continuum of HIV care targets[J]. HIV Med, 2017, 18(4):305-307. DOI: 10.1111/hiv.12431. 期刊类型引用(5)
1. 马红飞,龚舜,高代明,明方钊,张倩,刘恋,王继,王夏. 武汉市基层卫生服务机构人员开展艾滋病防治工作意愿调查. 医学动物防制. 2024(08): 816-821 .  百度学术
百度学术2. 吴修铭,袁风顺,袁丹,梁姝,卓玛拉措,陈卫中,刘伦皓. 2020年四川省艾滋病病毒检测发现情况及相关因素分析. 职业卫生与病伤. 2023(01): 1-6 . 百度学术3. 朱洋,何蔚云,魏丹诺,尤心怡,邓瑜,郝春,顾菁,郝元涛,韩志刚,李菁华. 应用诊断发现比简易数学模型估计广州市育龄女性中HIV感染者诊断比例. 中国艾滋病性病. 2022(02): 195-198 . 百度学术4. 金宇,崔莹,刘晓玲,黄怡丹. 2018—2021年成都市自愿咨询检测人群HIV确证阳性特征分析. 现代预防医学. 2022(12): 2281-2286 . 百度学术5. 张鹤美,高四海,李君,苏德华,赵丽娜,陈向阳,胡文雪,赖江宜,陈婉君. 2019年浙江省温州市艾滋病感染诊断治疗服务链特征分析. 疾病监测. 2022(08): 1063-1068 . 百度学术其他类型引用(3)
-

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 633
- HTML全文浏览量: 215
- PDF下载量: 77
- 被引次数: 8