

-
摘要:
目的 探究血脂水平与遗传因素在男性肿瘤发生中的作用。 方法 参照既往研究发表的肿瘤多基因风险评分,将英国生物样本库(UK Biobank, UKB)中的男性参与者根据遗传风险分为低、中及高三组;同时又以异常血脂指标数量作为标准,把研究对象分为三个类别,进而探究不同遗传风险下血脂水平与肿瘤发病风险的关联。 结果 研究共纳入178 171名男性作为研究对象,其中11 824人(6.64%)在随访期间新发肿瘤。在调整年龄、吸烟、饮酒以及空腹血糖等混杂因素后,血脂异常评分与肿瘤发病风险相关(均有P<0.001)。高遗传风险、高血脂异常评分人群的肿瘤发病风险是低遗传风险、低血脂异常评分人群的2.290倍(95% CI:2.039~2.571, P < 0.001)。 结论 在不同遗传风险人群中,血脂水平异常均可增加男性肿瘤发病风险。 Abstract:Objective To investigate the potential roles of blood lipid levels and genetic factors in cancer development in men. Methods Male participants in the UK Biobank (UKB) were stratified into low, intermediate and high genetic risk groups. The number of abnormal lipid levels was used to divide study subjects into three categories. The association between abnormal levels of blood lipid and the risk of cancer incidence under different genetic risks were analyzed. Results A total of 178 171 men were included in the study, of whom 11 824 (6.64%) developed new cancer cases within the follow-up period. After adjustment for confounders including age, smoking, alcohol consumption, and fasting plasma glucose, abnormal lipid score was associated with the risk of cancer (all P < 0.001). Men with high genetic risk and high lipid abnormal score had 2.290 fold higher (95% CI: 2.039-2.571, P < 0.001) overall cancer risk than those with low genetic risk and low lipid abnormal score. Conclusion Abnormal levels of blood lipid may increase the risk of cancer across different genetic risk groups in men. -
Key words:
- Blood lipids /
- Polygenic risk score /
- Cancer risk /
- Association
-

图 1 基于限制性立方样条模型分析血脂与肿瘤发病风险的关系a
注:a图中阴影部分为(95% CI)值范围。
Figure 1. Analysis on relationship between blood lipid and the risk of cancer based on restricted cubic spline model a

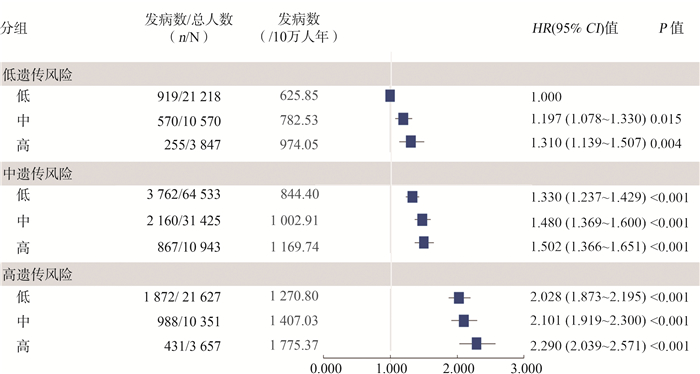
图 2 血脂异常评分与遗传因素对肿瘤发病风险的联合效应
Figure 2. Risk of cancer according to genetic factor and blood lipid categories
表 1 TC、HDL-C分级与肿瘤发病风险的关系a
Table 1. Risk of cancer according to levels defined by TC or HDL-C a
血脂指标 发病数(n) 总人数(N) HR(95% CI)值 P值 TC分组(组) Q1 3 621 44 576 1.079(1.033~1.126) 0.001 Q2~Q3 5 604 89 052 1.000 Q4 2 599 44 543 0.969(0.925~1.016) 0.189 HDL-C分组(组) Q1 3 203 44 664 1.113(1.064~1.163) <0.001 Q2~Q3 5 670 88 968 1.000 Q4 2 951 44 539 1.000(0.955~1.046) 0.994 注:a用Cox比例风险回归模型计算,调整年龄、受教育水平、BMI、空腹血糖、体力活动、家族史、汤森剥夺指数、吸烟、饮酒以及遗传背景。  下载: 导出CSV
下载: 导出CSV
表 2 血脂异常评分和肿瘤发病风险的关联a
Table 2. Risk of cancer according to risk levels defined by blood lipid a
血脂异常评分 发病数(n) 总人数(N) 随访时间(人年) HR(95% CI)值 P值 低 6 553 107 378 739 675 1.000 中 3 718 52 346 358 434 1.103(1.059~1.149) <0.001 高 1 553 18 447 124 575 1.155(1.090~1.225) <0.001 注:a用Cox比例风险回归模型计算,调整年龄、受教育水平、BMI、空腹血糖、体力活动、家族史、汤森剥夺指数、吸烟、饮酒以及遗传背景。
下载: 导出CSV
表 3 按遗传因素分层的血脂异常评分和肿瘤发病风险关联a
Table 3. Risk of cancer according to blood lipid categories within each genetic risk level a
分组 发病数/总人数(n/N) 发病数(/10万人年) HR(95% CI)值 P值 低遗传风险 低 919/21 218 625.85 1.000 中 570/10 570 782.53 1.175(1.057~1.307) 0.003 高 255/3 847 974.05 1.257(1.086~1.454) 0.002 中遗传风险 低 3 762/64 533 844.40 1.000 中 2 160/31 425 1 002.91 1.112(1.053~1.173) <0.001 高 867/10 943 1 169.74 1.125(1.041~1.215) 0.003 高遗传风险 低 1 872/21 627 1 270.80 1.000 中 988/10 351 1 407.03 1.054(0.974~1.140) 0.189 高 431/3 657 1 775.37 1.164(1.043~1.299) 0.007 注:a用Cox比例风险回归模型计算,调整年龄、受教育水平、BMI、空腹血糖、体力活动、家族史、汤森剥夺指数、吸烟、饮酒以及遗传背景。
下载: 导出CSV
-
[1] Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249. DOI: 10.3322/caac.21660. [2] Theodoratou E, Timofeeva M, Li X, et al. Nature, nurture, and cancer risks: genetic and nutritional contributions to cancer[J]. Annu Rev Nutr, 2017, 37: 293-320. DOI: 10.1146/annurev-nutr-071715-051004. [3] 隋小芳, 潘桂烨, 华玥祺, 等. 血脂异常的相关危险因素研究[J]. 中国实验诊断学, 2020, 24(5): 751-754. DOI: 10.3969/j.issn.1007-4287.2020.05.010.Sui XF, Hua YQ, Pan GY, et al. Study on related risk factors of dyslipidemia[J]. Chin J Lab Diagn, 2020, 24(5): 751-754. DOI: 10.3969/j.issn.1007-4287.2020.05.010. [4] Pelton K, Freeman MR, Solomon KR. Cholesterol and prostate cancer[J]. Curr Opin Pharmacol, 2012, 12(6): 751-759. DOI: 10.1016/j.coph.2012.07.006. [5] Ravnskov U, McCully KS, Rosch PJ. The statin-low cholesterol-cancer conundrum[J]. QJM, 2012, 105(4): 383-388. DOI: 10.1093/qjmed/hcr243. [6] Buniello A, MacArthur JAL, Cerezo M, et al. The NHGRI-EBI GWAS Catalog of published genome-wide association studies, targeted arrays and summary statistics 2019[J]. Nucleic Acids Res, 2019, 47(D1): D1005-D1012. DOI: 10.1093/nar/gky1120. [7] Jin G, Lv J, Yang M, et al. Genetic risk, incident gastric cancer, and healthy lifestyle: a meta-analysis of genome-wide association studies and prospective cohort study[J]. Lancet Oncol, 2020, 21(10): 1378-1386. DOI: 10.1016/s1470-2045(20)30460-5. [8] Dudbridge F. Polygenic epidemiology[J]. Genet Epidemiol, 2016, 40(4): 268-272. DOI: 10.1002/gepi.21966. [9] Dai J, Lv J, Zhu M, et al. Identification of risk loci and a polygenic risk score for lung cancer: a large-scale prospective cohort study in Chinese populations[J]. Lancet Respir Med, 2019, 7(10): 881-891. DOI: 10.1016/s2213-2600(19)30144-4. [10] Zhu M, Wang TP, Huang YQ, et al. Genetic risk for overall can-cer and the benefit of adherence to a healthy lifestyle[J]. Cancer Res, 2021. DOI: 10.1158/0008-5472.CAN-21-0836. [11] Bycroft C, Freeman C, Petkova D, et al. The UK Biobank resource with deep phenotyping and genomic data[J]. Nature, 2018, 562(7726): 203-209. DOI: 10.1038/s41586-018-0579-z. [12] Yang CH, Tian G, Mi J, et al. Causal relevance of circulating high-density lipoprotein cholesterol with cancer: a Mendelian randomization meta-analysis[J]. Sci Rep, 2015, 5: 9495. DOI: 10.1038/srep09495. [13] Lyu Z, Li N, Wang G, et al. Independent and joint associations of blood lipids and lipoproteins with lung cancer risk in Chinese males: a prospective cohort study[J]. Int J Cancer, 2019, 144(12): 2972-2984. DOI: 10.1002/ijc.32051. [14] Swanson KM, Hohl RJ. Anti-cancer therapy: targeting the mevalonate pathway[J]. Curr Cancer Drug Targets, 2006, 6(1): 15-37. DOI: 10.2174/156800906775471743. [15] Calleros L, Lasa M, Toro MJ, et al. Low cell cholesterol levels increase NFkappaB activity through a p38 MAPK-dependent mechanism[J]. Cell Signal, 2006, 18(12): 2292-2301. DOI: 10.1016/j.cellsig.2006.05.012. [16] von Eckardstein A, Hersberger M, Rohrer L. Current understanding of the metabolism and biological actions of HDL[J]. Curr Opin Clin Nutr Metab Care, 2005, 8(2): 147-152. DOI: 10.1097/00075197-200503000-00007. [17] Gurven M, Kaplan H, Winking J, et al. Inflammation and infection do not promote arterial aging and cardiovascular disease risk factors among lean horticulturalists[J]. PLoS One, 2009, 4(8): e6590. DOI: 10.1371/journal.pone.0006590. [18] Burger D, Dayer JM. High-density lipoprotein-associated apolipoprotein A-I: the missing link between infection and chronic inflammation?[J]. Autoimmun Rev, 2002, 1(1-2): 111-117. DOI: 10.1016/s1568-9972(01)00018-0. [19] Demacker PN, Schade RW, Jansen RT, et al. Intra-individual variation of serum cholesterol, triglycerides and high density lipoprotein cholesterol in normal humans[J]. Atherosclerosis, 1982, 45(3): 259-266. DOI: 10.1016/0021-9150(82)90227-1. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 618
- HTML全文浏览量: 297
- PDF下载量: 80
- 被引次数: 0