

Analysis for mortality trend and age-period-cohort of kidney cancer in China from 1990 to 2019
-
摘要:
目的 分析全球健康数据交换(the Global Health Data Exchange, GHDx)数据库中中国肾癌的死亡趋势及其流行病学特征。 方法 收集GHDx数据库中1990―2019年间20~<90岁中国人群肾癌死亡数据,运用Joinpoint回归模型分析肾癌死亡率的变化趋势,用年龄-时期-队列(age-period-cohort, APC)模型探讨影响肾癌死亡风险的年龄效应、时期效应与出生队列效应。 结果 1990―2019年全国、男性、女性肾癌标化死亡率均呈波动增长的趋势,平均年度变化百分比分别为2.04%、2.92%、0.70%;APC模型分析结果显示,无论男女,肾癌死亡风险均随着年龄的增长而增加,均随着时间的推移而增加,较晚出生的队列,其肾癌死亡风险均低于之前出生的队列。 结论 1990―2019年中国肾癌死亡率总体呈上升趋势,越早出生,年龄越大,生活在当代的人其肾癌死亡风险更高,肾癌造成的疾病负担仍是一个严重的公共卫生问题。 -
关键词:
- 肾癌 /
- 死亡率 /
- 变化趋势 /
- 年龄-时期-队列模型
Abstract:Objective To analyze the mortality trends and epidemiological characteristics of kidney cancer in China from the Global Health Data Exchange (GHDx) database. Methods We collected the kidney cancer mortality data in China among adults aged 20- < 90 years in GHDx database from 1990 to 2019. Joinpoint regression model was used to estimate the mortality trends. Age-period-cohort model was used to explore the age effect, period effect and cohort effect. Results The standardized mortality of kidney cancer from 1990 to 2019 showed a fluctuating growth trend in the whole population and the subgroups of male and female, with the average annual change percentage of 2.04%, 2.92% and 0.70% respectively; For both male and female, the relative risk of kidney cancer mortality increased with advancing age and time period, but decreased from earlier birth cohorts to more recent birth cohorts. Conclusions The overall trends of the mortality of kidney cancer in China increased from 1990 to 2019. People who born earlier, being older, and living in modern times have a higher risk of kidney cancer mortality. The disease burden caused by kidney cancer is still a serious public problem. -
Key words:
- Kidney neoplasms /
- Mortality /
- Trends /
- Age-period-cohort model
-

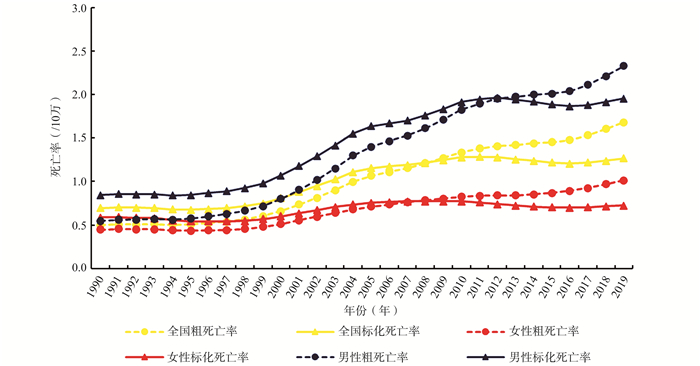
图 1 1990―2019年中国肾癌CMR和ASMR在全国、性别间的变化趋势
Figure 1. Trends of CMR and ASMR of kidney cancer in China from 1990 to 2019 among all the male and female group

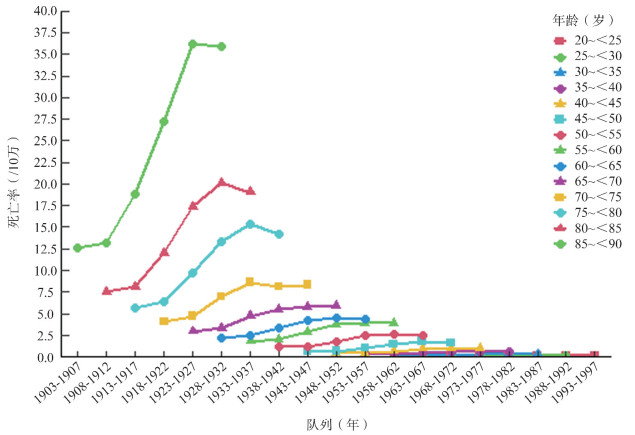
图 2 中国男性肾癌年龄别死亡率的队列趋势
Figure 2. Cohort trends on age-specific mortality of kidney cancer for male in China

图 3 中国女性肾癌年龄别死亡率的队列趋势
Figure 3. Cohort trends on age-specific mortality of kidney cancer for female in China

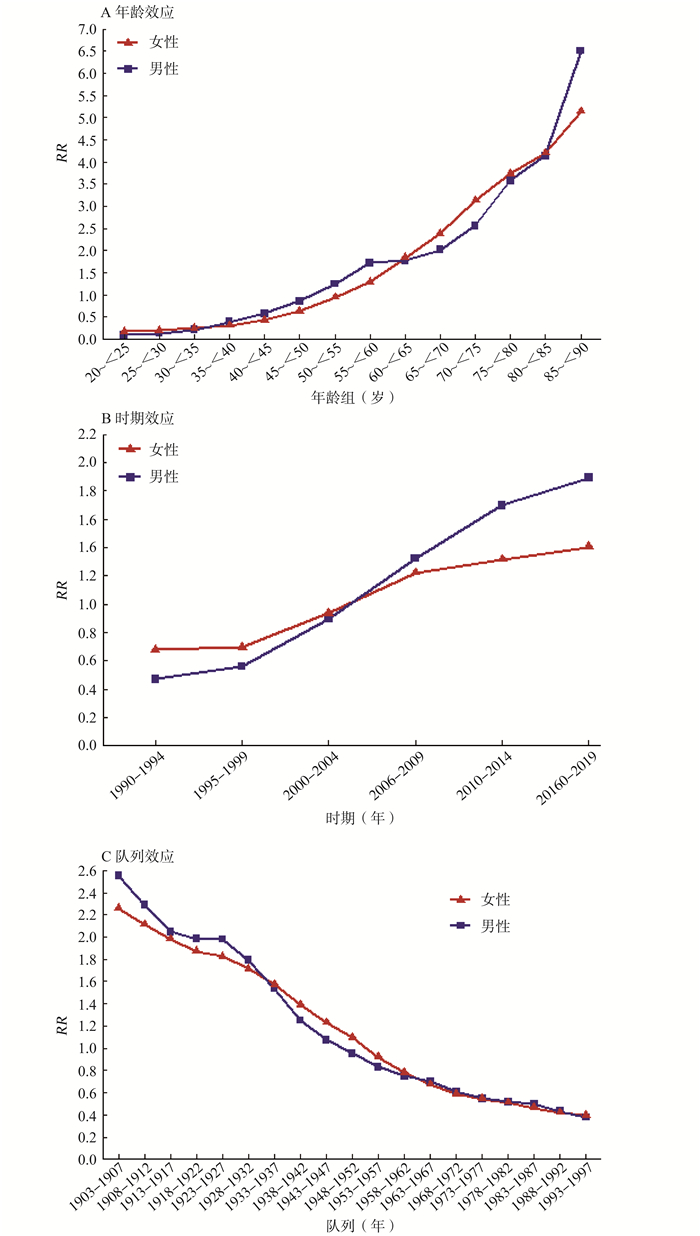
图 4 由不同效应引起的肾癌死亡率风险在性别之间的变化差异
Figure 4. Mortality relative risks of kidney cancer due to different effects, stratified by gender
表 1 1990―2019年中国肾癌ASMR的变化趋势
Table 1. Trends of ASMR of kidney cancer in China from 1990 to 2019
变量 ASMR(/10万) 1990年 2019年 年份 APC(95% CI)值 AAPC AAPC值 t值 P值 全国 0.70 1.27 1990―1996 -0.64(-0.98~-0.31) a 2.04 14.61 < 0.001 1996―1999 3.25(1.20~5.35) a 1999―2004 8.51(7.82~9.20) a 2004―2011 2.11(1.77~2.46) a 2011―2016 -1.51(-2.14~-0.89) a 2016―2019 1.71(0.69~2.73) a 女性 0.59 0.72 1990―1998 -1.21(-1.50~-0.92) a 0.70 5.34 < 0.001 1998―2004 5.67(5.03~6.32) a 2004―2009 0.87(0.01~1.75) a 2009―2016 -1.69(-2.15~-1.24) a 2016―2019 1.52(0.15~2.91) a 男性 0.85 1.96 1990―1996 0.08(-0.33~0.49) 2.92 16.73 < 0.001 1996―1999 4.50(2.00~7.07) a 1999―2004 9.87(9.03~10.71) a 2004―2011 3.34(2.92~3.76) a 2011―2017 -0.82(-1.35~-0.28) a 2017―2019 2.33(-0.12~4.84) 注:a表示P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 中国肾癌死亡率年龄-时期-队列模型分析结果
Table 2. Age-period-cohort (APC) model analysis results of kidney cancer mortality in China by gender
分组 男性 女性 效应系数 标准误 Z值 P值 效应系数 标准误 Z值 P值 年龄(岁) 20~<25 -2.37 1.50 -1.57 0.115 -1.78 1.65 -1.08 0.282 25~<30 -2.03 1.11 -1.83 0.068 -1.60 1.35 -1.19 0.233 30~<35 -1.52 0.87 -1.75 0.081 -1.40 1.19 -1.17 0.241 35~<40 -0.94 0.69 -1.36 0.174 -1.16 1.05 -1.11 0.267 40~<45 -0.55 0.59 -0.93 0.351 -0.83 0.89 -0.94 0.348 45~<50 -0.15 0.50 -0.30 0.761 -0.45 0.74 -0.62 0.538 50~<55 0.22 0.42 0.54 0.591 -0.05 0.61 -0.09 0.931 55~<60 0.55 0.35 1.58 0.114 0.26 0.50 0.52 0.600 60~<65 0.57 0.29 1.94 0.053 0.61 0.40 1.54 0.124 65~<70 0.70 0.24 2.89 0.004 0.87 0.33 2.68 0.007 70~<75 0.94 0.21 4.58 < 0.001 1.14 0.28 4.09 <0.001 75~<80 1.27 0.19 6.60 <0.001 1.32 0.28 4.71 <0.001 80~<85 1.42 0.22 6.47 <0.001 1.44 0.32 4.47 <0.001 85~<90 1.87 0.26 7.07 <0.001 1.64 0.39 4.19 <0.001 时期(年) 1990―1994 -0.76 0.24 -3.11 0.002 -0.39 0.32 -1.21 0.225 1995―1999 -0.58 0.18 -3.20 0.001 -0.36 0.24 -1.48 0.138 2000―2004 -0.11 0.13 -0.86 0.387 -0.07 0.18 -0.36 0.721 2005―2009 0.28 0.12 2.36 0.018 0.20 0.17 1.16 0.248 2010―2014 0.53 0.15 3.52 <0.001 0.27 0.22 1.25 0.212 2015―2019 0.64 0.20 3.17 0.002 0.34 0.29 1.18 0.239 队列(年) 1903―1907 0.94 0.48 1.93 0.053 0.81 0.66 1.24 0.217 1908―1912 0.83 0.39 2.13 0.033 0.75 0.52 1.44 0.150 1913―1917 0.72 0.32 2.28 0.023 0.68 0.42 1.63 0.102 1918―1922 0.68 0.26 2.66 0.008 0.63 0.34 1.83 0.067 1923―1927 0.68 0.22 3.13 0.002 0.60 0.29 2.05 0.041 1928―1932 0.58 0.20 2.85 0.004 0.54 0.28 1.92 0.055 1933―1937 0.43 0.24 1.78 0.075 0.45 0.33 1.35 0.176 1938―1942 0.22 0.30 0.75 0.451 0.33 0.41 0.80 0.424 1943―1947 0.07 0.36 0.20 0.844 0.21 0.50 0.42 0.678 1948―1952 -0.05 0.43 -0.11 0.909 0.09 0.60 0.15 0.877 1953―1957 -0.19 0.49 -0.38 0.706 -0.08 0.72 -0.12 0.907 1958―1962 -0.29 0.56 -0.51 0.608 -0.25 0.84 -0.30 0.766 1963―1967 -0.36 0.63 -0.56 0.572 -0.39 0.96 -0.41 0.681 1968―1972 -0.49 0.72 -0.68 0.495 -0.53 1.08 -0.49 0.628 1973―1977 -0.61 0.84 -0.73 0.468 -0.61 1.26 -0.48 0.628 1978―1982 -0.66 0.98 -0.68 0.500 -0.67 1.45 -0.46 0.644 1983―1987 -0.70 1.24 -0.56 0.575 -0.77 1.75 -0.44 0.660 1988―1992 -0.84 1.76 -0.48 0.634 -0.87 2.28 -0.38 0.704 1993―1997 -0.98 3.21 -0.30 0.761 -0.93 3.86 -0.24 0.809 AIC 3.46 2.86 BIC -212.22 -212.59 偏差 0.45 0.09 对数似然比 -109.31 -84.14 注:a表示P < 0.05。
下载: 导出CSV
-
[1] Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6): 394-424. DOI: 10.3322/caac.21492. [2] GBD Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1204-1222. DOI: 10.1016/s0140-6736(20)30925-9. [3] Cai QL, Chen YG, Qi XD, et al. Temporal trends of kidney cancer incidence and mortality from 1990 to 2016 and projections to 2030[J]. Transl Androl Urol, 2020, 9(2): 166-181. DOI: 10.21037/tau.2020.02.23. [4] Zhou MG, Wang HD, Zeng XY, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2019, 394(10204): 1145-1158. DOI: 10.1016/s0140-6736(19)30427-1. [5] 屈彦, 王天一, 杨津, 等. GBD数据库的数据提取方法与流程[J]. 中国循证心血管医学杂志, 2019, 11(9): 1043-1046. DOI: 10.3969/j.issn.1674-4055.2019.09.04.Qu Y, Wang TY, Yang J, et al. GBD database application and data extraction methods and processes[J]. Chin J Evid - Bases Cardiovasc Med, 2019, 11(9): 1043-1046. DOI: 10.3969/j.issn.1674-4055.2019.09.04. [6] GBD Demographics Collaborators. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950-2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1160-1203. DOI: 10.1016/s0140-6736(20)30977-6. [7] DeSantis CE, Miller KD, Dale W, et al. Cancer statistics for adults aged 85 years and older, 2019[J]. CA Cancer J Clin, 2019, 69(6): 452-467. DOI: 10.3322/caac.21577. [8] Yang Y, Fu WJ, Land KC. A methodological comparison of age-period-cohort models: the intrinsic estimator and conventional generalized linear models[J]. Sociol Methodol, 2004, 34(1): 75-110. DOI: 10.1111/j.0081-1750.2004.00148.x. [9] 苏晶晶, 彭非. 年龄-时期-队列模型参数估计方法最新研究进展[J]. 统计与决策, 2014, 419(23): 21-26. DOI: 10.13546/j.cnki.tjyjc.2014.23.005.Su JJ, Peng F. Recent progress in age-period-cohort model parameter estimation methods[J]. Statistics & Decision, 2014, 419(23): 21-26. DOI: 10.13546/j.cnki.tjyjc.2014.23.005. [10] Sung WW, Ko PY, Chen WJ, et al. Trends in the kidney cancer mortality-to-incidence ratios according to health care expenditures of 56 countries[J]. Sci Rep, 2021, 11(1): 1479. DOI: 10.1038/s41598-020-79367-y. [11] Mohammadian M, Pakzad R, Towhidi F, et al. Incidence and mortality of kidney cancer and its relationship with HDI (Human Development Index) in the world in 2012[J]. Clujul Med, 2017, 90(3): 286-293. DOI: 10.15386/cjmed-691. [12] 刘呈军, 聂富强, 任栋. 高质量发展背景下我国人类发展指数协调性测度[J]. 统计与决策, 2021, 37(5): 60-64. DOI: 10.13546/j.cnki.tjyjc.2021.05.012.Liu CJ, Nie FQ, Ren D. Coordination measure of Chinese human development index under the background of high-quality development[J]. Statistics & Decision, 2021, 37(5): 60-64. DOI: 10.13546/j.cnki.tjyjc.2021.05.012. [13] Manton KG, Akushevich I, Kravchenko J. Cancer mortality and morbidity patterns in the US population[M]. New York, NY: Springer New York, 2009. [14] Sims JN, Yedjou CG, Abugri D, et al. Racial disparities and preventive measures to renal cell carcinoma[J]. Int J Environ Res Public Health, 2018, 15(6): e1089. DOI: 10.3390/ijerph15061089. [15] Rosenberg PS. A new age-period-cohort model for cancer surveillance research[J]. Stat Methods Med Res, 2019, 28(10-11): 3363-3391. DOI: 10.1177/0962280218801121. [16] Chen WQ, Xia CF, Zheng RS, et al. Disparities by province, age, and sex in site-specific cancer burden attributable to 23 potentially modifiable risk factors in China: a comparative risk assessment[J]. Lancet Glob Health, 2019, 7(2): e257-e269. DOI: 10.1016/S2214-109X(18)30488-1. [17] Hofmann F, Hwang EC, Lam TB, et al. Targeted therapy for metastatic renal cell carcinoma[J]. Cochrane Database Syst Rev, 2020, 10: CD012796. DOI: 10.1002/14651858.cd012796.pub2. [18] 王健, 赵凯. 中国城镇化、老龄化、城乡差距与经济发展研究: 基于有调节的中介效应模型[J]. 当代经济管理, 2020, 42(7): 49-58. DOI: 10.13253/j.cnki.ddjjgl.2020.07.007.Wang J, Zhao K. Urbanization, aging, urban-rural gap and economic development in China—a moderated mediation model[J]. Contemp Econ Manag, 2020, 42(7): 49-58. DOI: 10.13253/j.cnki.ddjjgl.2020.07.007. [19] Liu XX, Zhou MG, Wang F, et al. Secular trend of cancer death and incidence in 29 cancer groups in China, 1990-2017: a joinpoint and age-period-cohort analysis[J]. Cancer Manag Res, 2020, 12: 6221-6238. DOI: 10.2147/cmar.S247648. [20] 杨莹. 现阶段中国居民的营养与健康[J]. 农村经济与科技, 2014, 25(8): 56-57. DOI: 10.3969/j.issn.1007-7103.2014.08.021.Yang Y. Nutrition and health of Chinese residents at present[J]. Rural Econ Sci - Technol, 2014, 25(8): 56-57. DOI: 10.3969/j.issn.1007-7103.2014.08.021. [21] Sanfilippo KM, McTigue KM, Fidler CJ, et al. Hypertension and obesity and the risk of kidney cancer in 2 large cohorts of US men and women[J]. Hypertension, 2014, 63(5): 934-941. DOI: 10.1161/hypertensionaha.113.02953. [22] Labochka D, Moszczuk B, Kukwa W, et al. Mechanisms through which diabetes mellitus influences renal cell carcinoma development and treatment: a review of the literature[J]. Int J Mol Med, 2016, 38(6):1887-1894. DOI: 10.3892/ijmm.2016.2776. [23] Washio M, Mori M, Mikami K, et al. Cigarette smoking and other risk factors for kidney cancer death in a Japanese population: Japan Collaborative Cohort Study for evaluation of cancer risk (JACC study)[J]. Asian Pac J Cancer Prev, 2014, 14(11):6523-6528. DOI: 10.7314/apjcp.2013.14.11.6523. [24] Liu XX, Yu Y, Wang MS, et al. Age-period-cohort analysis of kidney cancer deaths attributable to high body-mass index in China and US. adults[J]. BMC Public Heal, 2020, 20(1):1-10. DOI: 10.1186/s12889-020-09007-7. [25] 佟明坤, 满塞丽麦, 金成, 等. 千万例体检人群高血压患病率、知晓率、治疗率和控制率的调查[J]. 中国循环杂志, 2020, 35(9):866-872. DOI: 10.3969/j.issn.1000-3614.2020.09.004.Tong MK, Man S, Jin C, et al. Prevalence, awareness, treatment and control of hypertension in China: survey on a 10 million health check-up population[J]. Chin Circ J, 2020, 35(9):866-872. DOI: 10.3969/j.issn.1000-3614.2020.09.004. [26] 谢朴仙. 健康体检人群超重肥胖的分布情况及健康干预[J]. 中国社区医师, 2018, 34(22):169, 171. DOI: 10.3969/j.issn.1007-614x.2018.22.106.Xie PX. Distribution and health intervention of overweight and obesity in physical examination population[J]. Chin Community Dr, 2018, 34(22):169, 171. DOI: 10.3969/j.issn.1007-614x.2018.22.106. [27] 陈川, 黄育北, 刘雪鸥, 等. 中国5个地区45 ~ 65岁女性吸烟及被动吸烟现况分析[J]. 中华流行病学杂志, 2014, 35(7):797-801. DOI: 10.3760/cma.j.issn.0254-6450.2014.07.009.Chen C, Huang YB, Liu XO, et al. Current status of smoking and passive smoking among aged 45 to 65 years old females in five cities of China[J]. Chin J Epidemiol, 2014, 35(7):797-801. DOI: 10.3760/cma.j.issn.0254-6450.2014.07.009. [28] Chen WQ, Liang ZH, Cen HS, et al. Status and development of tumor registration in China[J]. Chin J Front Med Sci Electron Version, 2016, 8(7):1-5. DOI: 10.3969/j.issn.1674-7372.2016.07.001. [29] Reither EN, Hauser RM, Yang Y. Do birth cohorts matter? Age-period-cohort analyses of the obesity epidemic in the United States[J]. Soc Sci Med, 2009, 69(10):1439-1448. DOI: 10.1016/j.socscimed.2009.08.040. [30] Fogel RW, Costa DL. A theory of technophysio evolution, with some implications for forecasting population, health care costs, and pension costs[J]. Demography, 1997, 34(1):49-66. http://web.mit.edu/14.731/www/theory.pdf [31] Godfrey KM, Barker DJ. Fetal nutrition and adult disease[J]. Am J Clin Nutr, 2000, 71(5 Suppl):1344s-1352s. DOI: 10.1093/ajcn/71.5.1344s. [32] 王昱政, 胡樱. 1992—2016年中国肾癌死亡趋势的年龄-时期-队列分析[J]. 中华流行病学杂志, 2021, 42(3):508-512. DOI: 10.3760/cma.j.cn112338-20200224-00156.Wang YZ, Hu Y. Age-period-cohort analysis on kidney cancer mortality trend in China, 1992-2016[J]. Chin J Epidemiol, 2021, 42(3):508-512. DOI: 10.3760/cma.j.cn112338-20200224-00156. [33] 李春晖. 中国20-84岁女性乳腺癌死亡趋势及年龄-时期-队列模型的研究[D]. 武汉:武汉大学, 2015.Li CH. The study of breast cancer mortality trends and age-period-cohort model among 20-84 years old Chinese female[D]. Wuhan: Wuhan University, 2015. -


 点击查看大图
点击查看大图
计量
- 文章访问数: 1053
- HTML全文浏览量: 622
- PDF下载量: 242
- 被引次数: 0