

Three types of treatment delay and influencing factors among Multidrug-resistant Tuberculosis patients in Guizhou Province, 2014-2020
-
摘要:
目的 分析贵州省2014―2020年耐多药结核病(multidrug-resistant tuberculosis, MDR-TB)患者三类治疗延迟现况及影响因素。 方法 从“结核病管理信息系统”中收集患者信息;趋势χ2检验分析率随时间变化趋势;χ2检验和多因素logistic回归分析模型用于延迟因素分析。根据患者治疗延迟天数将其分为三类:第I类(延迟>1 d)、第II类(延迟>7 d)和第III类(延迟>14 d)。 结果 2014―2020年贵州省登记的1 309例MDR-TB患者中第I、II和III类治疗延迟率分别为43.6%、30.0%和22.7%。三类延迟率均随时间变化呈总体下降趋势(均有P<0.001)。但2019年12月―2020年延迟率较以往有所升高,其中2019年12月延迟率最高达47%;2020年总体延迟率较2019年上升。农民、有固定职业、来自毕节市诊疗机构、采用传统药物敏感性试验诊断、既往接受过抗结核病治疗和确诊时住院治疗的患者更容易发生延迟(均有P<0.05)。 结论 贵州省2014―2020年MDR-TB患者三类治疗延迟率均较高,虽呈逐年下降趋势,但自2019年12月起延迟率较以往有所升高。职业、诊疗机构、诊断方式、抗结核病治疗史和确诊时治疗模式是患者治疗延迟的影响因素,应采取综合措施以降低治疗延迟的发生。 Abstract:Objective To analyze the status and influencing factors for three types of treatment delay among multidrug-resistant tuberculosis (MDR-TB) patients in Guizhou Province from 2014 to 2020. Methods Data were collected from the TB Management Information System. χ2 trend test was adopted to analyze the rate with time change, meanwhile, univariate analysis with χ2 test and multivariate logistic regression analysis were performed to obtain the influencing factors for treatment delay. Participants were classified into three types based on the days of their treatment delay, including type I (>1 day), type II (>7 days) and type III (>14 days). Results The treatment delay rates of type I, II and III among 1 309 MDR-TB patients in Guizhou Province from 2014 to 2020 were 43.6%, 30.0% and 22.7%, respectively. The three types of delay rates showed an overall downward trend with the change of time (all P-values were less than 0.001). However, the delay rate from December 2019 to 2020 was higher than that before, and the highest rate was 47% in December 2019. The overall delay rate increased in 2020 compared with that in 2019. Patients who were farmers, had fixed occupations, were diagnosed with MDR-TB and received treatment in hospital in Bijie City, were diagnosed through traditional drug sensitivity test, received anti-TB treatment in the past and were hospitalized at the time of MDR-TB diagnosis were more likely to experience treatment delay (all P < 0.05). Conclusions The three types of treatment delay rates of MDR-TB patients are high in Guizhou Province from 2014 to 2020. Although the delay rates show a downward trend year by year, they have increased since December 2019. Meanwhile, occupation, diagnosis and treatment institution, diagnosis mode, and anti-TB treatment history and treatment mode at the time of diagnosis are the influencing factors for treatment delay. Comprehensive measures should be taken to reduce the occurrence of treatment delay in Guizhou. -
Key words:
- Multidrug-resistant tuberculosis /
- Treatment delay /
- Influencing factors
-

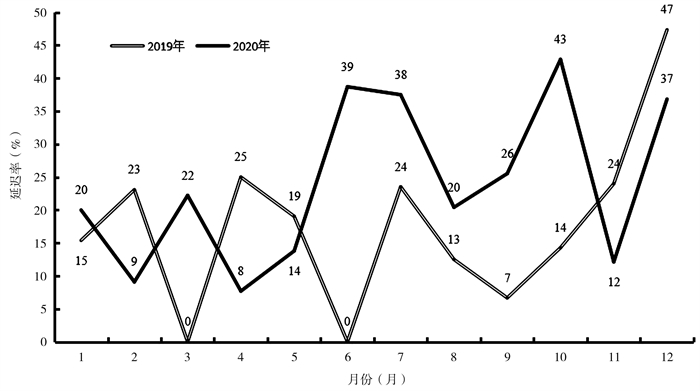
图 1 贵州省2019年与2020年MDR-TB患者第III类治疗延迟率分月比较
Figure 1. Comparison of type III of treatment delay among MDR-TB patients in Guizhou Province in 2019 and 2020 by month

图 2 贵州省不同地区诊疗机构收治的MDR-TB患者治疗延迟率及不同DST检测方法比例的情况比较
注:a黔铜六(3州市)为黔西南州、铜仁市和六盘水市的简称。
Figure 2. Comparison of treatment delay and proportion detected by different DST methods among MDR-TB patients admitted to medical institutions in different regions of Guizhou Province
表 1 2014―2020年贵州省MDR-TB患者的三类治疗延迟发生率及随时间变化趋势[n(%)]
Table 1. Three types of treatment delays with time change among MDR-TB patients in Guizhou Province from 2014 to 2020 [n(%)]
年份(年) 患者总数(例) 第I类治疗延迟 第II类治疗延迟 第III类治疗延迟 2014 86 67(77.9) 54(62.8) 44(51.2) 2015 128 75(58.6) 49(38.3) 31(24.2) 2016 161 98(60.9) 55(34.2) 39(24.2) 2017 183 61(33.3) 38(20.8) 28(15.3) 2018 169 61(36.1) 41(24.3) 27(16.0) 2019 227 81(35.7) 59(26.0) 43(18.9) 2020 355 128(36.1) 97(27.3) 85(23.9) 合计 1 309 571(43.6) 393(30.0) 297(22.7) χ趋势2值 98.1 62.5 52.3 P值 <0.001 <0.001 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 贵州省MDR-TB患者基本情况及其与三类治疗延迟关联的单因素分析结果[n(%)]
Table 2. The basic information of MDR-TB patients in Guizhou Province and their association with three types of treatment delay by univariate analysis [n(%)]
变量 患者数(例) 第I类 第II类 第III类 延迟 χ2值 P值 延迟 χ2值 P值 延迟 χ2值 P值 性别 0.09 0.760 0.02 0.876 0.43 0.511 女 392(29.9) 174(44.4) 116(29.6) 94(24.0) 男 917(70.1) 397(43.3) 277(30.2) 203(22.1) 年龄(岁) 6.79 0.034 1.08 0.583 2.01 0.365 <26 262(20.0) 98(37.4) 72(27.5) 53(20.2) 26~<60 866(66.2) 399(46.1) 264(30.5) 197(22.7) ≥60 181(13.8) 74(40.0) 57(31.5) 47(26.0) 民族 0.43 0.510 2.08 0.150 3.98 0.046 汉族 1 100(84.0) 475(43.2) 321(29.2) 238(21.6) 少数民族 209(16.0) 96(45.9) 72(34.4) 59(28.2) 职业 49.50 < 0.001 19.40 < 0.001 20.15 < 0.001 学生 45(3.4) 16(35.6) 11(24.4) 8(17.8) 工人 675(51.6) 236(35.0) 169(25.0) 122(18.1) 固定职业 49(3.7) 23(46.9) 19(38.8) 16(32.7) 农民 540(41.3) 296(54.8) 194(35.9) 151(28.0) 抗结核病治疗史 2.54 0.281 6.22 0.045 12.76 0.002 未使用过抗结核病药 50(3.8) 19(38.0) 13(26.0) 6(12.0) 用过一线抗结核病药 1 181(90.2) 512(43.4) 347(29.4) 262(22.2) 用过一线和二线抗结核病药 78(6.0) 40(51.3) 33(42.3) 29(37.2) DST检测方法 154.96 < 0.001 213.96 < 0.001 206.35 < 0.001 快速 991(75.7) 336(33.9) 193(19.5) 131(13.2) 传统 318(24.3) 235(73.9) 200(62.9) 166(52.2) 治疗模式 59.38 < 0.001 44.03 < 0.001 28.56 < 0.001 门诊 1 000(76.4) 377(37.7) 253(25.3) 192(19.2) 住院 309(23.6) 194(62.8) 140(45.3) 105(34.0) 合计 1 309(100.0) 571(43.6) 393(30.0) 297(22.7)
下载: 导出CSV
表 3 影响贵州省MDR-TB患者三类治疗延迟的多因素分析结果
Table 3. Results of influencing factors for three types of treatment delay among MDR-TB patients in Guizhou Province by multivariate analysis
变量 第I类 第II类 第III类 ORadj(95% CI)值 P值 ORadj(95% CI)值 P值 ORadj(95% CI)值 P值 年龄(岁) <26 1.00 0.089 26~<60 1.37(1.00~1.89) ≥60 1.08(0.70~1.67) 民族 汉族 1.00 0.415 1.00 0.414 少数民族 1.14(0.83~1.57) 1.18(0.80~1.73) 职业 学生 1.00 < 0.001 < 0.001 0.010 工人 1.10(0.55~2.20) 1.01(0.50~2.06) 0.98(0.44~2.22) 固定职业 1.43(0.58~3.54) 1.94(1.08~4.77) 2.07(1.17~5.57) 农民 2.04(1.02~4.07) 1.66(1.01~3.39) 1.50(1.06~3.36) 诊疗机构所在州(市) 贵阳市 1.00 0.002 1.00 0.022 1.00 0.044 黔东南州 0.79(0.48~1.31) 1.19(0.69~2.06) 1.43(0.81~2.52) 黔铜六(3州市) a 0.51(0.25~1.04) 1.20(0.59~2.45) 1.54(0.74~3.20) 遵义市 1.19(0.56~2.55) 1.34(0.95~1.88) 1.07(0.73~1.57) 毕节市 1.70(1.22~2.35) 3.00(1.49~6.03) 2.85(1.41~5.76) 抗结核病治疗史 未使用过抗结核病药 1.00 0.078 1.00 0.010 用过一线抗结核病药 1.08(0.56~2.08) 2.19(0.90~5.35) 用过一线和二线抗结核病药 1.86(0.84~4.11) 4.01(1.47~10.94) DST检测方法 快速 1.00 < 0.001 1.00 < 0.001 1.00 < 0.001 传统 4.94(3.62~6.72) 7.10(5.21~9.68) 8.37(6.03~11.63) 治疗模式 门诊 1.00 < 0.001 1.00 < 0.001 1.00 0.078 住院 2.62(1.95~3.51) 1.78(1.30~2.44) 1.37(0.97~1.94) 注:a黔铜六(3州市)为黔西南州、铜仁市和六盘水市的简称。
下载: 导出CSV
-
[1] 曾伟. 安徽省巢湖市新发现肺结核病人诊治延迟影响因素及控制对策研究[D]. 合肥: 安徽医科大学, 2011.Zeng W. Study on influencing factors and controlling strategy of delay in consultation, diagnosis and treatment of new tuberculosis patients in Chaohu city of Anhui province[D]. Hefei: Anhui Medical University, 2011. [2] 周成超. 山东省流动人口肺结核病人求医行为及治疗管理现状与对策研究[D]. 济南: 山东大学, 2011.Zhou CC. Study on current status and counter measures of Tuberculosis patients health seeking behavior and treatment management among migrants in Shandong[D]. Jinan: Shandong University, 2011. [3] 张思源, 黄飞, 汪彦辉, 等. 家庭收入与新发涂阳肺结核诊治延迟的关系[J]. 南京医科大学学报(社会科学版), 2015, 15(1): 39-42. DOI: 10.7655/NYDXBSS20150110.Zhang SY, Hang F, Wang YH, et al. Relationship between family income and delayed diagnosis and treatment of new smear positive tuberculosis[J]. Acta Univ Med Nanjing (Soc Sci), 2015, 15(1): 39-42. DOI: 10.7655/NYDXBSS20150110. [4] 赵秀秀, 徐凌忠, 郭振, 等. 山东省肺结核病人治疗延迟情况及影响因素分析[J]. 中国卫生统计, 2013, 30(2): 187-189. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWT201302008.htmZhao XX, Xu LZ, Guo Z, et al. Analysis of treatment delay and influencing factors of pulmonary tuberculosis patients in Shandong province[J]. Chin J Heal Stat, 2013, 30(2): 187-189. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWT201302008.htm [5] Yang Q, Tong Y, Yin X, et al. Delays in care seeking, diagnosis and treatment of patients with pulmonary tuberculosis in Hubei, China[J]. Int Health, 2020, 12(2): 101-106. DOI: 10.1093/inthealth/ihz036. [6] 谢显扬, 姚若兴, 杨达书, 等. 2010-2014年平远县肺结核流行病学分析[J]. 疾病监测与控制杂志, 2015, 9(12): 843-845. https://www.cnki.com.cn/Article/CJFDTOTAL-JBJK201512001.htmXie XY, Yao RX, Yang DS, et al. Epidemiological analysis of tuberculosis in Pingyuan County between 2010 and 2014[J]. J Diseases Monitor & Control, 2015, 9(12): 843-845. https://www.cnki.com.cn/Article/CJFDTOTAL-JBJK201512001.htm [7] 孔荣, 陈亮, 黄致信. 初治涂阳肺结核社会经济学调查及延误治疗的相关因素分析[J]. 现代预防医学, 2020, 47(1): 88-92. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYF202001027.htmKong R, Chen L, Huang ZX. Socioeconomics of new smear -positive pulmonary tuberculosis and related factors of delayed treatment[J]. Mod Prev Med, 2020, 47(1): 88-92. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYF202001027.htm [8] 中国防痨协会. 耐药结核病化学治疗指南(2019年简版)[J]. 中国防痨杂志, 2019, 41(10): 1025-1073. DOI: 10.3969/j.issn.1000-6621.2019.10.001.Chinese Antituberculosis Association. Guidelines for Chemotherapy of Multidrug-resistant tuberculosis (Simplified version 2019)[J]. Chin J Antituberc, 2019, 41(10): 1025-1073. DOI: 10.3969/j.issn.1000-6621.2019.10.001. [9] 曹德明, 石华, 郭微媛. 结核分枝杆菌快速药敏实验的研究进展[J]. 国际检验医学杂志, 2011, 32(11): 1204-1206. DOI: 10.3969/j.issn.1673-4130.2011.11.028.Cao DM, Shi H, Guo WY. Research progress on rapid drug sensitivity test of Mycobacterium tuberculosis[J]. Int J Lab Med, 2011, 32(11): 1204-1206. DOI: 10.3969/j.issn.1673-4130.2011.11.028. [10] 何琳, 唐诗邈, 曹宏伟, 等. 2012-2017年辽宁省耐多药结核病患者特征分析[J]. 中国卫生工程学, 2020, 19(1): 22-25. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWX202001008.htmHe L, Tang SM, Cao HW, et al. Analysis of Multidrug-resistant tuberculosis patient's characteristics from 2012 to 2017 in Liaoning Province[J]. Chin J Public Heal Eng, 2020, 19(1): 22-25. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWX202001008.htm [11] 贵州省卫生厅. 贵州省卫生厅关于印发《贵州省新农合终末期肾病等6种重大疾病按病种付费实施方案(试行)》的通知[EB/OL]. (2013-02-27)[2021-05-16]. http://www.gzzhijin.gov.cn/zxfw/msztfw/ylws/jzzc/201710/t20171016_24857461.html.Guizhou Provincial Health Bureau. The implementation plan of quota payment of specific diseases in the new rural cooperative medical system for 6 major diseases including end-stage renal disease and others in Guizhou Province issued by Guizhou Provincial Health Bureau[EB/OL]. (2013-02-27)[2021-05-16]. http://www.gzzhijin.gov.cn/zxfw/msztfw/ylws/jzzc/201710/t20171016_24857461.html. [12] 严非. 中国结核病控制现状、问题与对策-社会评价案例研究[D]. 上海: 复旦大学, 2007.Yan F. Current situation and strategy or tuberculosis control in China-social assessment study in four provinces[D]. Shanghai: Fudan University, 2007. [13] Ying L, John Ehiri, Sheng LT, et al. Factors associated with patient and diagnostic delays in Chinese TB patients: a systematic review and meta-analysis[J]. BMC Med, 2013, 11: 156. DOI: 10.1186/1741-7015-11-156. [14] Storla DG, Yimer S, Bjune GA. A systematic review of delay in the diagnosis and treatment of tuberculosis[J]. BMC Public Health, 2008, 8: 15. DOI: 10.1186/1471-2458-8-15. -


 点击查看大图
点击查看大图
计量
- 文章访问数: 318
- HTML全文浏览量: 125
- PDF下载量: 45
- 被引次数: 0