

Analysis of prevalence and determinants of chronic obstructive pulmonary disease in rural Yunnan Province based on structure equation modeling
-
摘要:
目的 分析云南省农村居民慢性阻塞性肺疾病(chronic obstructive pulmonary disease,COPD)患病现况及其影响因素。 方法 采用多阶段分层随机抽样方法抽取云南省农村地区7 572名≥35岁常住居民进行现场问卷调查和体格检查,采用主成分分析法(principal component analysis,PCA)构建个体社会经济地位(socioeconomic status,SES),运用结构方程模型(structure equation modeling,SEM)分析COPD患病的影响因素。 结果 云南省农村居民COPD患病率为12.60%,男性患病率高于女性(χ2 =57.973,P<0.001);COPD患病率随年龄的增加而升高(χ趋势2=165.616,P<0.001);少数民族居民COPD患病率高于汉族居民(χ2=33.785,P<0.001);SES越低,COPD患病率越高(χ趋势2=10.751,P<0.001)。SEM分析结果显示,性别、年龄、民族和SES对COPD患病具有直接和间接作用,其总路径系数分别为0.09、0.15、0.06和-0.05,而COPD家族史、低BMI、现在吸烟和被动吸烟对COPD患病只有直接作用, 其路径系数分别为0.06、0.03、0.08和0.08。 结论 云南省农村居民COPD患病率较高,应加强对男性、高龄、吸烟、低BMI、有COPD家族史和SES较低人群的COPD健康教育和干预工作。 Abstract:Objective The aim of this study was to analyze the prevalence and determinants of chronic obstructive pulmonary disease (COPD) in rural areas of Yunnan Province. Methods The multi-stage stratified random sampling method was used to conduct on-site questionnaire survey and physical examination among 7 572 rural residents aged ≥35 years from three counties in Yunnan Province. Principal component analysis was used to construct individual socioeconomic status (SES). Structure Equation Modeling (SEM) was used to analyze possible influencing factors of prevalence of COPD. Results Among the study population, the prevalence of COPD was 12.60%. Males had a significantly higher prevalence of COPD than females (15.54% and 9.73%, χ2 =57.973, P < 0.001). Prevalence of COPD increased with age (χtrend2=165.616, P < 0.001). Ethnic minority groups had a higher prevalence of COPD than Han majority (χtrend2=33.785, P < 0.001). Individuals with lower SES had a higher prevalence of COPD than their counterparts (χ2 =10.751, P < 0.001). The results of SEM analysis indicated that the following associated factors had both direct and indirect statistically significant effect on prevalence of COPD: gender (0.09), age (0.15), ethnicity (0.06), and SEP (-0.05) had both direct and indirect effects on prevalence of COPD, whereas family history of COPD (0.06), low BMI (0.03), current smoking (0.08), and passive smoking (0.08) only directly associated with prevalence of COPD. Conclusions The prevalence of COPD is high in rural Yunnan Province. Future health education and intervention to prevent and control COPD should focus on males, elderly people, current smokers, individuals with low BMI, and individuals with family history of COPD and low SES. -

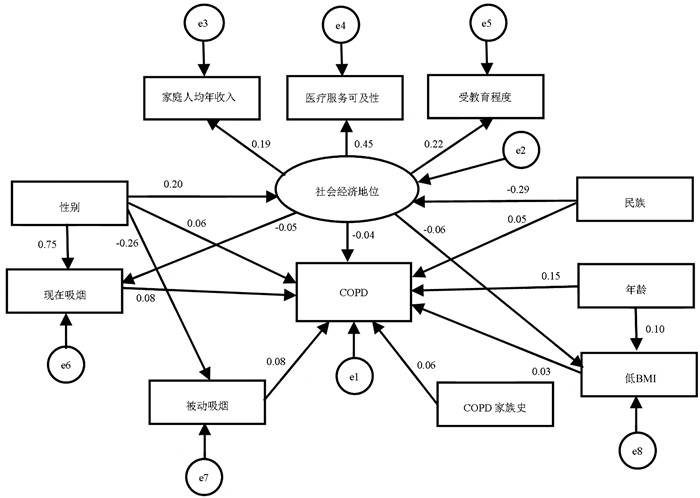
图 1 云南省农村居民COPD患病影响因素的结构方程模型
Figure 1. Structure equation modeling on determinants of COPD in rural Yunnan Province
表 1 云南省农村居民SES的PCA
Table 1. PCA of SES among rural residents in Yunnan
统计指标 数值 KMO统计值 0.700 Bartlett's球形检验 近似χ2值 122.768 P值 <0.001 特征根 1.149  下载: 导出CSV
下载: 导出CSV
表 2 云南省农村居民分性别、民族的SES分布情况[n(%)]
Table 2. Distribution of SES by sex and ethnicity in rural Yunnan Province [n(%)]
组别 SES分组 χ2值 P值 低 中等偏下 中等偏上 高 性别 4.628 <0.001 男 826 (22.09) 860 (23.00) 987 (26.40) 1 066(28.51) 女 1 037 (27.05) 955 (24.92) 1 039(27.11) 802(20.92) 民族 3.914 <0.001 汉族 932 (22.60) 960 (23.28) 1 218 (29.53) 1 014(24.59) 少数民族 931 (27.00) 855 (24.80) 808 (23.43) 854(24.77) 合计 1 863 (24.60) 1 815 (23.97) 2 026 (26.76) 1 868(24.67)
下载: 导出CSV
表 3 云南省农村居民分性别、民族的SES分布情况
Table 3. Distribution of SES by sex and ethnicity in rural Yunnan Province
组别 患病人数(n) 患病率(%) χ2值 P值 组别 患病人数(n) 患病率(%) χ2值 P值 性别 57.973 <0.001 SES 11.777 0.008 男 581 15.54 低 259 13.9 女 373 9.73 中等偏下 251 13.83 年龄组(岁) 171.386 <0.001 中等偏上 243 11.99 35~<45 83 6.61 高 201 10.76 45~<55 167 8.77 COPD家族史 23.519 <0.001 55~<65 223 12.02 是 22 31.88 65~<75 284 17.01 否 932 12.42 ≥75 197 22.26 低BMI 22.308 <0.001 民族 33.785 <0.001 是 77 20.48 汉族 436 10.57 否 877 12.19 少数民族 518 15.02 现在吸烟 72.668 <0.001 受教育程度 4.146 0.032 是 479 16.78 文盲 241 13.93 否 475 10.07 小学及以上 713 12.2 被动吸烟 34.204 <0.001 家庭年人均收入 15.422 <0.001 是 251 17.16 低 541 14.07 否 703 11.51 高 413 11.08 医疗服务可及性 4.904 0.028 差 333 13.68 好 621 12.09
下载: 导出CSV
表 4 云南省农村居民COPD患病影响因素的SEM的拟合度
Table 4. The fit of the SEM of determinants of COPD in rural Yunnan Province
统计检验量 适配标准或临界值 最终模型指标 拟合度 绝对适配度指数 良适性适配指数 >0.90 0.998 符合 调整后良适性适配指数 >0.90 0.995 符合 渐进残差均方和平方根 < 0.08(适配合理) < 0.05(适配良好) 0.017 适配良好 残差均方和平方根 < 0.05 0.003 符合 增值适配度指数 规准适配指数 >0.90 0.989 符合 相对适配指数 >0.90 0.977 符合 增值适配指数 >0.90 0.993 符合 非规准适配指数 >0.90 0.984 符合 比较适配指数 >0.90 0.993 符合 简约适配度指数 临界样本数 >200 3 475 符合 一致性赤池信息量准则值 理论模型小于独立模型,且小于饱和模型 482.01<655.53<8 026.08 符合
下载: 导出CSV
表 5 各变量对COPD患病的直接、间接作用及作用路径系数
Table 5. Direct and indirect effects and path coefficients of each variable on COPD
组别 直接作用 路径系数 间接作用 路径系数 总路径系数 性别 性别→COPD 0.06 a 性别→SES、现在吸烟、被动吸烟→COPD 0.03 a 0.09 a 年龄(岁) 年龄→COPD 0.15 a 年龄→低BMI→COPD 0.003 a 0.15 a 民族 民族→COPD 0.05 a 民族→SES→COPD 0.01 a 0.06 a 受教育程度 SES→COPD -0.01 b -0.01 b 家庭人均年收入 SES→COPD -0.01 b -0.01 b 医疗服务可及性 SES→COPD -0.02 b -0.02 b SES SES→COPD -0.04 b SES→低BMI、现在吸烟、被动吸烟→COPD -0.01 b -0.05 b COPD家族史 COPD家族史→COPD 0.06 a 0.06 a 低BMI 低BMI→COPD 0.03 a 0.03 a 现在吸烟 现在吸烟→COPD 0.08 a 0.08 a 被动吸烟 被动吸烟→COPD 0.08 a 0.08 a 注: aP<0.001; bP<0.05。
下载: 导出CSV
-
[1] 中华医学会呼吸病学分会慢性阻塞性肺疾病学组, 中国医师协会呼吸医师分会慢性阻塞性肺疾病工作委员会. 慢性阻塞性肺疾病诊治指南(2021年修订版)[J]. 中华结核和呼吸杂志, 2021, 44(3): 170-205. DOI: 10.3760/cma.j.cn112147-20210109-00031.Chronic Obstructive Pulmonary Disease Committee, Respiratory Society, Chinese Medical Association. Guidelines for the diagnosis and management of chronic obstructive pulmonary disease (revised version 2021)[J]. Chin J Tuberc Respir Dis, 2021, 44(3): 170-205. DOI: 10.3760/cma.j.cn112147-20210109-00031. [2] Zhong NS, Wang C, Yao WZ, et al. Prevalence of chronic obstructive pulmonary disease in China: a large, population-based survey[J]. Am J Respir Crit Care Med, 2007, 176(8): 753-760. DOI: 10.1164/rccm.200612-1749OC. [3] Wang C, Xu JY, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health[CPH] Study): a national cross-sectional study[J]. Lancet, 2018, 391(10131): 1706-1717. DOI: 10.1016/S0140-6736(18)30841-9. [4] 李凡, 孙惠芬, 段静, 等. 从GOLD指南的演变看慢性阻塞性肺疾病的防治[J]. 中国全科医学, 2019, 22(27): 3275-3280. DOI: 10.12114/j.issn.1007-9572.2019.00.383.Li F, Sun HF, Duan J, et al. Prevention and treatment of chronic obstructive pulmonary disease from the evolution of GOLD[J]. Chin Genl Pract, 2019, 22(27): 3275-3280. DOI: 10.12114/j.issn.1007-9572.2019.00.383. [5] 卞玉梅. 结构方程模型研究及其应用[D]. 大连: 大连海事大学, 2017.Bian YM. Research and application of structural equation model[D]. Dalian: DalianMaritime University, 2017. [6] 吴明隆. 结构方程模型[M]. 重庆: 重庆大学出版社, 2013: 1-53.Wu ML. Structural Equation Model[M]. Chongqing: Chongqing University Press, 2013: 1-53. [7] 云南省统计局. 云南统计年鉴-2019(总第35期)[M]. 北京: 中国统计出版社, 2019: 23-29.Yunnan Bureau of statistics. Yunnan statistical yearbook 2019[M]. Beijing: China Statistics Press, 2019: 23-29. [8] Cai L, Wang XM, Fan LM, et al. Socioeconomic disparities in prevalence and behaviors of smoking in rural Southwest China[J]. BMC Public Health, 2019, 19(1): 1117. DOI: 10.1186/S12889-019-7455-0. [9] 中国肥胖问题工作组. 中国成人超重和肥胖症预防与控制指南(节录)[J]. 营养学报, 2004, 26(1): 1-4. DOI: 10.13325/j.cnki.acta.nutr.sin.2004.01.001.China Obesity Task Group. Guidelines for prevention and control of overweight and obesity in Chinese adults (Excerpt)[J]. Acta Nutrimenta Sinica, 2004, 26(1): 1-4. DOI: 10.13325/j.cnki.acta.nutr.sin.2004.01.001. [10] 金航, 章文强, 马新雅, 等. 四川省城乡慢性阻塞性肺病患病率及影响因素分析[J]. 预防医学情报杂志, 2021, 37(4): 465-471, 477. https://www.cnki.com.cn/Article/CJFDTOTAL-YFYX202104006.htmJin H, Zhang WQ, Ma XY, et al. Prevalence and Influencing Factors of Chronic Obstructive Pulmonary Disease in Urban and Rural Areas of Sichuan Province[J]. J Prev Med Inf, 2021, 37(4): 465-471, 477. https://www.cnki.com.cn/Article/CJFDTOTAL-YFYX202104006.htm [11] 罗倩, 王晓园, 张海涛, 等. 新疆乌鲁木齐市城乡40岁以上居民慢性阻塞性肺疾病的患病情况与相关危险因素分析[J]. 临床肺科杂志, 2019, 24(9): 1562-1567. DOI: 10.3969/j.issn.1009-6663.2019.09.003.Luo Q, Wang XY, Zhang HT, et al. Analysis on the prevalence and risk factors of chronic obstructive pulmonary disease among urban and rural residents over 40 years old in Urumqi Xinjiang[J]. Journal of Clinical Pulmonary Medicine, 2019, 24(9): 1562-1567. DOI: 10.3969/j.issn.1009-6663.2019.09.003. [12] 黄鑫, 王波. 2019—2020年成都地区慢性阻塞性肺疾病患病特征及影响因素[J]. 公共卫生与预防医学, 2020, 31(5): 68-71. DOI: 10.3969/j.issn.1006-2483.2020.05.018.Huang X, Wang B. Prevalence characteristics and influencing factors of COPD in Chengdu, 2019-2020[J]. J of Pub Heal Prev Med, 2020, 31(5): 68-71. DOI: 10.3969/j.issn.1006-2483.2020.05.018. [13] Cockerham WC. Health lifestyle theory and the convergence of agency and structure[J]. J Health Soc Behav, 2005, 46(1): 51-67. DOI: 10.1177/002214650504600105. [14] 李潇, 蔡乐, 王旭明, 等. 云南省农村老年人五种常见慢性病及共病的流行现状及与社会经济地位的关系[J]. 中华疾病控制杂志, 2019, 23(6): 630-634. DOI: 10.16462/j.cnki.zhjbkz.2019.06.003.Li X, Cai L, Wang XM, et al. The prevalence of five common chronic diseases and multi-morbidity and its relationship with socioeconomic position among rural older adults in Yunnan Province[J]. Chin J Dis Control Prev, 2019, 23(6): 630-634. DOI: 10.16462/j.cnki.zhjbkz.2019.06.003. [15] Gershon AS, Warner L, Cascagnette P, et al. Lifetime risk of developing chronic obstructive pulmonary disease: a longitudinal population study[J]. Lancet, 2011, 378(9795): 991-996. DOI: 10.1016/S0140-6736(11)60990-2. [16] 夏翠翠, 李建新. 社会经济地位对中老年人口慢性疾病患病的影响分析——以心脑血管疾病和慢性呼吸系统疾病为例[J]. 人口学刊, 2018, 40(3): 82-92. DOI: 10.16405/j.cnki.1004-129X.2018.03.008.Xia CC, Lin JX. Influence of socioeconomic status on the middle aged and elderly's chronic non-infectious disease in China: the case of cardiovascular disease and chronic respiratory disease[J]. Popul J, 2018, 40(3): 82-92. DOI: 10.16405/j.cnki.1004-129X.2018.03.008. [17] 王辰, 肖丹, 池慧. 《中国吸烟危害健康报告2020》概要[J]. 中国循环杂志, 2021, 36(10): 937-952. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGXH202110001.htmWang C, Xiao D, Chi H. 2020 report on health hazards of smoking in China: an updated summary[J]. Chin Circu J, 2021, 36(10): 937-952. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGXH202110001.htm [18] Vorrink SN, Kort HS, Troosters T, et al. Level of daily physical activity in individuals with COPD compared with healthy controls[J]. Respir Res, 2011, 12(1): 33. DOI: 10.1186/1465-9921-12-33. [19] Siddharthan T, Grigsby MR, Goodman D, et al. Association between household air pollution exposure and chronic obstructive pulmonary disease outcomes in 13 low- and middle-lncome country settings[J]. Am J Respir Crit Care Med, 2018, 197(5): 611-620. DOI: 10.1164/rccm.201709-1861OC. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 266
- HTML全文浏览量: 123
- PDF下载量: 32
- 被引次数: 0