

The correlation of serum S100A8 level and the prognosis in patients with community-acquired pneumonia
-
摘要:
目的 分析社区获得性肺炎(community-acquired pneumonia, CAP)患者入院时血清S100钙结合蛋白A8(S100 calcium-binding protein A8, S100A8)水平与预后之间的关联,并探讨血清S100A8升高的可能危险因素。 方法 收集2018年12月―2020年12月在亳州市人民医院就诊的CAP患者临床信息和血清样本,用酶联免疫吸附试验(enzyme-linked immunosorbent assay, ELISA)检测血清S100A8和炎症因子的水平。 结果 最终招募100名符合条件的CAP患者。随着入院时血清S100A8水平的升高,CAP患者住院时间延长(F=23.562, P=0.005)。期间有10名CAP患者死亡,死亡组血清S100A8水平高于存活组(t=4.352, P=0.004)。logistic回归分析模型分析发现血清S100A8升高是住院时间延长(OR=3.111, 95% CI: 1.112~8.702, P=0.031)和死亡率增加(OR=1.214, 95% CI: 1.058~1.562, P=0.022)的危险因素。Pearson关联性分析发现S100A8水平与炎症因子水平呈正相关。进一步logistic回归分析模型分析发现,年龄(OR=1.230, 95% CI: 1.030~1.528, P=0.044)、高SBP(OR=1.155, 95% CI: 1.011~1.320, P=0.033)以及合并肾脏疾病(OR=2.541, 95% CI: 1.578~6.537, P=0.038)均是CAP患者血清S100A8升高的独立危险因素。 结论 CAP患者入院时血清S100A8水平与不良预后呈正相关,血压升高、合并肾脏疾病的CAP老年患者血清S100A8更易升高。血清S100A8水平可能作为CAP患者预后的一个早期诊断分子标志物。 -
关键词:
- 社区获得性肺炎 /
- S100钙结合蛋白A8 /
- 住院时间 /
- 死亡风险 /
- 炎症
Abstract:Objective To explore the correlation between serum S100A8 on admission and the prognosis in patients with community-acquired pneumonia (CAP) as well as the potential risk factors of S100A8 elevation. Methods CAP patients were enrolled from December 2018 to December 2020 in the Department of Respiratory and Critical Care Medicine of Bozhou People's Hospital. Demographic characteristics and clinical information were extracted. Serum samples were collected. The levels of S100A8 and inflammatory cytokines were measured using enzyme-linked immunosorbent assay. Results All 100 patients with CAP were enrolled. The hospital stay was increased in parallel with serum S100A8 on admission among CAP patients (F=23.562, P=0.005). In addition, 10 patients with CAP died during hospitalization. Serum S100A8 level was higher in dead patients than those in alive cases (t=4.352, P=0.004). Moreover, logistic regression analysis found that serum S100A8 elevation was the risk factor of hospital stay prolonging (OR=3.111, 95% CI: 1.112-8.702, P=0.031) and mortality elevation (OR=1.214, 95% CI: 1.058-1.562, P=0.022) in CAP patients. Additionally, Pearson correlation analysis found that S100A8 level was associated with inflammatory cytokines. Further logistic regression analysis found that age (OR=1.230, 95% CI: 1.030-1.528, P=0.044), high systolic pressure (OR=1.155, 95% CI: 1.011-1.320, P=0.033) and comorbidity with renal disease (OR=2.541, 95% CI: 1.578-6.537, P=0.038) were independent risk factors of S100A8 elevation among CAP patients. Conclusions Serum S100A8 level on admission is positively correlated with adverse prognosis in CAP patients. Serum S100A8 is more prone to elevating in older and higher blood pressure patients with renal disease. Consequently, S100A8 may be used as an early serum biomarker of prognosis for CAP patients. -
Key words:
- Community-acquired pneumonia /
- S100A8 /
- Hospital stay /
- Death risk /
- Inflammation
-

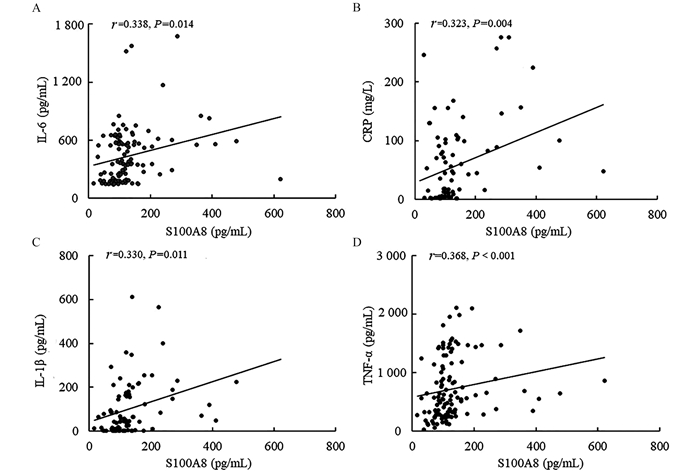
图 1 不同CAP患者入院时S100A8水平
注:A表示不同住院时间的CAP患者S100A8水平(<8 d组,n=35;8~14 d,n=34;>14 d组,n=31);B表示存活和死亡CAP患者S100A8水平(存活组,n=90;死亡组,n=10);a表示P < 0.05。
Figure 1. The levels of serum S100A8 in the different CAP patients on admission

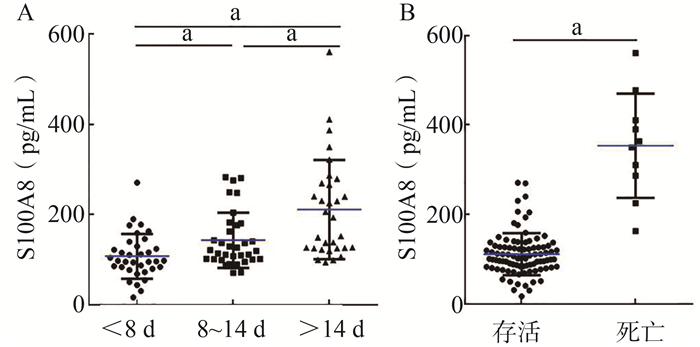
图 2 入院时S100A8水平与炎症因子之间的关联
注:A表示S100A8与IL-6之间的相关性;B表示S100A8与CRP之间的相关性;C表示S100A8与IL-1β之间的相关性;D表示S100A8与TNF-α之间的相关性。
Figure 2. The associations between serum S100A8 and informatory cytokines on admission
表 1 人口学特征和临床信息
Table 1. Demographic characteristics and clinical information
变量 S100A8<中位数(n=50) S100A8≥中位数(n=50) χ2/t/Z值 P值 年龄(x±s, 岁) 59.52±2.73 67.98±2.47 5.295 0.024 性别 4.058 0.044 男性[n(%)] 23(41.1) 33(58.9) 女性[n(%)] 27(61.4) 17(38.6) BMI(x±s, kg/m2) 22.64±0.59 23.04±0.62 0.203 0.654 SBP(x±s, mm Hg) 123.96±2.76 121.56±2.99 0.347 0.557 DBP(x±s, mm Hg) 74.84±1.47 72.00±1.49 1.849 0.177 白细胞数(x±s, ×109/L) 7.07±0.54 9.47±0.92 4.930 0.029 中性粒细胞数(x±s, ×109/L) 6.35±1.44 7.53±0.89 5.148 0.026 淋巴细胞数(x±s, ×109/L) 3.68±0.23 1.24±0.095 0.157 0.079 肌酐(x±s, μmol/L) 4.75±0.23 7.37±0.61 16.657 0.001 尿素氮(x±s, mmol/L) 57.46±2.59 79.31±9.16 5.452 0.022 尿酸(x±s, μmol/L) 275.40±12.96 283.06±19.61 0.108 0.743 谷丙转氨酶(x±s, U/L) 29.66±3.57 26.77±4.09 0.285 0.595 谷草转氨酶(x±s, U/L) 31.10±3.13 32.71±3.16 0.131 0.718 降钙素原[M(P25, P75), ng/mL] 0.04(0.02, 0.11) 0.20(0.06, 1.05) 3.121 0.082 D-二聚体[M(P25, P75), μg/mL] 3.94(1.56, 6.58) 6.69(5.11, 10.56) 2.214 0.015 C反应蛋白(x±s, mg/mL) 46.16±9.17 70.69±10.36 2.860 0.095 IL-6(x±s, pg/mL) 76.89±15.65 185.65±25.69 3.498 0.047 TNF-α(x±s, pg/mL) 424.35±55.28 895.63±46.25 1.301 0.025 IL-1β(x±s, pg/mL) 169.85±25.63 425.65±58.35 6.359 0.013 并发症 糖尿病[n(%)] 6(12.0) 5(10.0) 0.102 0.749 高血压[n(%)] 10(20.0) 11(22.0) 0.060 0.806 肺源性心脏病[n(%)] 1(2.0) 7(14.0) 4.891 0.027 间质性肺炎[n(%)] 5(10.0) 4(8.0) 0.122 0.727 慢性阻塞性肺疾病[n(%)] 1(2.0) 5(10.0) 2.837 0.092 肝脏疾病[n(%)] 8(16.0) 11(22.0) 0.585 0.444 肾脏疾病[n(%)] 6(12.0) 2(4.0) 2.174 0.140 心血管疾病[n(%)] 6(12.0) 14(28.0) 4.000 0.046 脑部疾病[n(%)] 6(12.0) 12(26.0) 2.439 0.118 严重性评分[M(P25, P75), 分] CURB-65 1.0(0.0, 2.0) 2.0(1.0, 4.0) -5.013 < 0.001 CRB-65 1.0(0.0, 2.0) 2.0(1.0, 3.0) -4.574 < 0.001 PSI 78.50(45.00, 109.30) 116.00(79.00, 168.00) -3.962 < 0.001 CURXO [n(%)] 13(26.0) 27(54.0) 8.167 0.004 SMART-COP[M(P25, P75), 分] 1.00 (0.00, 2.30) 4.00 (1.00, 7.00) -3.861 < 0.001  下载: 导出CSV
下载: 导出CSV
表 2 CAP患者血清S100A8的水平(x±s)
Table 2. The levels of serum S100A8 in CAP patients (x±s)
变量 例数 S100A8(pg/mL) t/Z/F值 P值 变量 例数 S100A8(pg/mL) t/Z/F值 P值 年龄(岁) 3.654 0.013 并发症 < 50 23 78.65±8.65 间质性肺炎 0.321 0.098 50~ < 60 30 98.35±10.51 是 9 112.35±15.65 ≥60 47 133.65±12.35 否 91 106.39±10.65 性别 6.365 < 0.001 慢性阻塞性肺疾病 5.697 0.002 男 56 96.56±7.65 是 6 156.32±12.65 女 44 75.69±8.69 否 94 96.35±8.97 并发症 肝脏疾病 0.874 0.214 糖尿病 0.635 0.312 是 19 89.65±12.65 是 11 102.35±15.65 否 81 112.36±18.74 否 89 103.36±10.45 肾脏疾病 7.954 0.003 高血压 1.354 0.024 是 8 146.35±12.67 是 21 135.62±11.35 否 92 87.98±8.91 否 79 89.64±8.97 心血管疾病 7.654 < 0.001 肺源性心脏病 0.368 0.748 是 20 155.68±13.65 是 8 101.35±8.64 否 80 101.78±10.48 否 92 93.35±12.67 脑部疾病 0.412 0.158 是 18 91.05±15.65 否 82 102.25±14.65
下载: 导出CSV
表 3 S100A8水平与CAP患者预后之间的关联
Table 3. The associations between serum S100A8 and prognosis in CAP patients
变量 OR(95% CI)值 P值 OR(95% CI)值a P值 死亡(例) 1.132(1.013~1.552) <0.001 1.214(1.058~1.562) 0.022 住院时间(d) <8 1.000 1.000 8~14 0.571(0.200~1.628) 0.294 0.825(0.315~2.161) 0.696 >14 2.038(1.674~4.168) 0.025 3.111(1.112~8.702) 0.031 注:a表示调整年龄和性别。
下载: 导出CSV
表 4 CAP患者血清S100A8升高的危险因素
Table 4. The risk factors of serum S100A8 elevation in CAP patients
变量 单因素分析 多因素分析 β值 Wald值 OR(95% CI)值 P值 β值 Wald值 OR(95% CI)值 P值 年龄(岁) -0.025 4.903 1.256(1.018~1.568) 0.027 0.030 1.368 1.230(1.030~1.528) 0.044 男性 0.824 3.999 2.279(1.017~5.108) 0.046 -1.491 2.495 0.225(0.035~1.432) 0.114 BMI(kg/m2) -0.036 0.209 0.965(0.829~1.124) 0.648 SBP(mm Hg) 0.006 0.351 1.764(1.122~3.542) 0.002 0.144 4.528 1.155(1.011~1.320) 0.033 DBP(mm Hg) 0.027 1.822 1.027(0.988~1.067) 0.177 糖尿病(例) -0.066 0.012 0.936(0.281~3.121) 0.914 高血压(例) 0.158 0.107 1.171(0.455~3.014) 0.744 肺源性心脏病(例) -2.009 3.406 0.134(0.016~1.133) 0.065 间质性肺炎(例) 0.308 0.193 1.361(0.344~5.387) 0.660 慢性阻塞性肺疾病(例) 1.121 2.245 2.121(1.121~4.356) 0.018 18.810 1.214 2.562(0.589~5.214) 0.254 肝脏疾病(例) -0.430 0.719 0.651(0.241~1.759) 0.087 肾脏疾病(例) 1.246 2.191 3.477(2.145~6.254) 0.022 -39.215 3.251 2.541(1.578~6.537) 0.038 心血管疾病(例) 1.063 4.001 2.895(1.022~8.202) 0.045 -1.515 0.690 0.220(0.006~7.833) 0.406 脑部疾病(例) 0.968 3.271 2.632(0.922~7.515) 0.071
下载: 导出CSV
-
[1] Franco J. Community-acquired pneumonia[J]. Radiol Technol, 2017, 88(6): 621-636. [2] Bartlett JG, Mundy LM. Community-acquired pneumonia[J]. N Engl J Med, 1995, 333(24): 1618-1624. DOI: 10.1056/nejm199512143332408. [3] Lim WS, Baudouin SV, George RC, et al. BTS guidelines for the management of community acquired pneumonia in adults: update 2009[J]. Thorax, 2009, 64(Suppl 3): iii1-iii55. DOI: 10.1136/thx.2009.121434. [4] Ferreira-Coimbra J, Sarda C, Rello J. Burden of community-acquired pneumonia and unmet clinical needs[J]. Adv Ther, 2020, 37(4): 1302-1318. DOI: 10.1007/s12325-020-01248-7. [5] He GY, Zhao CH, Wu DG, et al. S100A8 promotes inflammation via toll-like receptor 4 after experimental traumatic brain injury[J]. Front Neurosci, 2020, 14: 616559. DOI: 10.3389/fnins.2020.616559. [6] Xiao X, Yang C, Qu SL, et al. S100 proteins in atherosclerosis[J]. Clin Chim Acta, 2020, 502: 293-304. DOI: 10.1016/j.cca.2019.11.019. [7] Boyd JH, Kan B, Roberts H, et al. S100A8 and S100A9 mediate endotoxin-induced cardiomyocyte dysfunction via the receptor for advanced glycation end products[J]. Circ Res, 2008, 102(10): 1239-1246. DOI: 10.1161/CIRCRESAHA.107.167544. [8] Ruan G, Xu J, Wang K, et al. Associations between serum S100A8/S100A9 and knee symptoms, joint structures and cartilage enzymes in patients with knee osteoarthritis[J]. Osteoarthritis Cartilage, 2019, 27(1): 99-105. DOI: 10.1016/j.joca.2018.08.020. [9] Azramezani Kopi T, Amini Kadijani A, Parsian H, et al. The value of mRNA expression of S100A8 and S100A9 as blood-based biomarkers of inflammatory bowel disease[J]. Arab J Gastroenterol, 2019, 20(3): 135-140. DOI: 10.1016/j.ajg.2019.07.002. [10] Huang XL, Tan XY, Liang Y, et al. Differential DAMP release was observed in the sputum of COPD, asthma and asthma-COPD overlap (ACO) patients[J]. Sci Rep, 2019, 9(1): 19241. DOI: 10.1038/s41598-019-55502-2. [11] Raquil MA, Anceriz N, Rouleau P, et al. Blockade of antimicrobial proteins S100A8 and S100A9 inhibits phagocyte migration to the alveoli in streptococcal pneumonia[J]. J Immunol, 2008, 180(5): 3366-3374. DOI: 10.4049/jimmunol.180.5.3366. [12] Unamuno X, Gómez-Ambrosi J, Ramírez B, et al. NLRP3 inflammasome blockade reduces adipose tissue inflammation and extracellular matrix remodeling[J]. Cell Mol Immunol, 2021, 18(4): 1045-1057. DOI: 10.1038/s41423-019-0296-z. [13] Fujita Y, Khateb A, Li Y, et al. Regulation of S100A8 stability by RNF5 in intestinal epithelial cells determines intestinal inflammation and severity of colitis[J]. Cell Rep, 2018, 24(12): 3296-3311.e6. DOI: 10.1016/j.celrep.2018.08.057. [14] Zheng L, Fei J, Feng CM, et al. Serum 8-iso-PGF2α predicts the severity and prognosis in patients with community-acquired pneumonia: a retrospective cohort study[J]. Front Med (Lausanne), 2021, 8: 633442. DOI: 10.3389/fmed.2021.633442. [15] Liu HY, Xiang HX, Xiang Y, et al. The associations of serum S100A9 with the severity and prognosis in patients with community-acquired pneumonia: a prospective cohort study[J]. BMC Infect Dis, 2021, 21(1): 327. DOI: 10.1186/s12879-021-06020-y. [16] Huang YK, Liu AH, Liang L, et al. Diagnostic value of blood parameters for community-acquired pneumonia[J]. Int Immunopharmacol, 2018, 64: 10-15. DOI: 10.1016/j.intimp.2018.08.022. [17] 傅利军, 黄朝辉, 屠春雨, 等. 儿童社区获得性肺炎住院时间的影响因素分析[J]. 中华疾病控制杂志, 2015, 19(1): 99-101. DOI: 10.16462/j.cnki.zhjbkz.2015.01.030.Fu LJ, Huang ZH, Tu CY, et al. Factors associated with duration of hospital stays in community acquired pneumonia of children[J]. Chin J Dis Control Prev, 2015, 19(1): 99-101. DOI: 10.16462/j.cnki.zhjbkz.2015.01.030. [18] Fu L, Li XY, Fei J, et al. Myocardial injury at early stage and its association with the risk of death in COVID-19 patients: a hospital-based retrospective cohort study[J]. Front Cardiovasc Med, 2020, 7: 590688. DOI: 10.3389/fcvm.2020.590688. [19] Fu L, Fei J, Xu S, et al. Liver dysfunction and its association with the risk of death in COVID-19 patients: a prospective cohort study[J]. J Clin Transl Hepatol, 2020, 8(3): 246-254. DOI: 10.14218/JCTH.2020.00043. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 641
- HTML全文浏览量: 293
- PDF下载量: 41
- 被引次数: 0