

-
摘要:
目的 探讨绝经前后血尿酸(serum uric acid, SUA)水平变化。 方法 基于开滦体检队列,用线性和分段线性混合效应模型分析绝经前后SUA变化,并分析基线年龄和基线BMI分别与绝经前后时间分段的相乘交互作用。 结果 2006—2020年的7次体检共3 747例女性,共21 223人次体检记录被纳入分析。首次体检平均年龄为(46.19±4.11)岁,中位绝经年龄为51.00(50.00, 53.00)岁。与绝经前相比,绝经后SUA水平升高10.15 μmol/L。SUA从绝经前11年开始缓慢增加,平均年增长量为1.99 μmol/L;绝经前5~前2年每年平均增加3.30 μmol/L;SUA在绝经前后2年的平均年增长量为4.60 μmol/L;随后平均年增长量下降,在绝经5年后,平均年增长量降至1.77 μmol/L。基线年龄 < 40岁与绝经后2~ < 5年(Pinteraction=0.009)和绝经≥5年(Pinteraction < 0.001)的时间分段存在交互作用,基线年龄40~ < 45岁与绝经前后2年时间有交互作用(Pinteraction=0.033);除基线年龄 < 40岁对绝经2年后SUA变化有影响,其他基线年龄组SUA在绝经前后的变化一致。基线BMI与绝经前后各时间分段均无交互作用(均Pinteraction>0.05)。 结论 绝经对SUA有不良影响,中年女性在绝经前后应关注SUA水平,采取积极防控策略。 Abstract:Objective To investigate the changes of serum uric acid (SUA) around menopause. Methods The linear and piecewise linear mixed effect models were used to analyze SUA changes in the pre-and post-menopause on the Kailuan Health Examination cohort. Multiplicative interaction effects between baseline age as well as baseline BMI and segmented time periods pre- and post-menopause were also analyzed. Results A total of 3 747 female with 21 223 health examination records from 2006 to 2020 (7 health examinations) were included in the analysis. The average age at the first health examination was (46.19 ± 4.11) years, and the median age at menopause was 51(50, 53) years. Compared to pre-menopause, SUA increased by 10.15 μmol/L in post-menopause. SUA started to increase gradually from 11 years before menopause, with an average annual increase of 1.99 μmol/L; From 5 to 2 years before menopause, SUA increased by an average of 3.30 μmol/L per year; During the 2 years before and after menopause period, SUA increased by an average of 4.60 μmol/L per year. After that, the average annual increase slowed, and after 5 years of menopause, the average annual increase in SUA dropped to 1.77 μmol/L. There was an interaction between baseline age < 40 years and the time segments of postmenopausal 2- < 5 years after menopause (Pinteraction=0.009) and 5 years or more after menopause (Pinteraction < 0.001), as well as between baseline age 40- < 45 years and the 2 years before and after menopause (Pinteraction=0.033). Except for age under 40 years, which had an impact on SUA changes during 2 years after menopause, the SUA changes around menopause in other baseline age groups were consistent. There was no multiplication interaction effect between baseline BMI and various time segments around menopause (all Pinteraction>0.05). Conclusions Menopause has an adverse effect on SUA. Middle-aged women should pay attention to their SUA levels around menopause and adopt proactive prevention and control strategies. -
Key words:
- Menopause /
- Serum uric acid /
- Cohort study /
- Body mass index
-

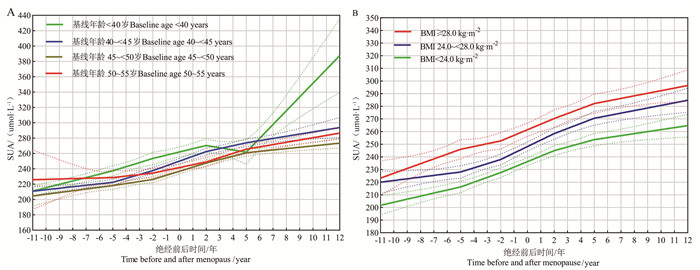
图 1 不同基线年龄组(A)和不同基线BMI组(B)女性绝经前后SUA的分段线性混合效应模型拟合图
SUA:血尿酸。
Figure 1. Fitting graph of piece-wise linear mixed effect model for SUA before and after menopause in women according to different baseline age groups (A) and baseline BMI groups (B)
SUA: serum uric acid.
表 1 研究队列信息
Table 1. The information of study cohort
队列信息The information of cohort 第1次体检The first examination 第2次体检The second examination 第3次体检The third examination 第4次体检The fourth examination 第5次体检The fifth examination 第6次体检The sixth examination 第7次体检The seventh examination 参加当次体检人数Number of participants in the current examination 3 746 3 160 3 340 3 229 2 948 2 901 3 080 缺失当次体检人数Missing of participants in the current examination 0 586 406 517 798 845 666 因SUA缺失而剔除的记录数Number of records excluded due to missing SUA 304 77 60 82 87 156 415 纳入分析的记录数Number of records included in the analysis 3 442 3 083 3 280 3 147 2 861 2 745 2 665 注:SUA, 血尿酸。
Note: SUA, serum uric acid. 下载: 导出CSV
下载: 导出CSV
表 2 研究对象各次体检特征
Table 2. Characteristics of participants at each examination
变量Variable 第1次体检The first examination 第2次体检The second examination 第3次体检The third examination 第4次体检The fourth examination 第5次体检The fifth examination 第6次体检The sixth examination 第7次体检The seventh examination 记录数Records 3 442 3 083 3 280 3 147 2 861 2 745 2 665 年龄/岁Age/years, x±s 46.19±4.11 47.73±4.59 49.45±4.68 51.71±4.68 53.82±4.76 56.42±4.56 57.89±4.49 教育程度Education level 高中以下① Below senior high school ① 2 392(69.53) 2 055(66.66) 2 202(67.13) 2 105(66.89) 1 926(67.58) 1 918(69.9) 1 769(66.43) 高中及以上① Senior high school or above ① 1 048(30.47) 1 028(33.34) 1 078(32.87) 1 042(33.11) 924(32.42) 826(30.10) 894(33.57) 缺失人数Missing 2 0 0 0 1 1 2 基线吸烟状态① Baseline smoking status ① 不吸烟No smoking 3 388(98.43) 3 033(98.38) 3 233(98.57) 3 099(98.47) 2 828(98.85) 2 707(98.62) 2 634(98.84) 既往吸烟Previous smoking 9(0.26) 9(0.29) 8(0.24) 8(0.25) 6(0.21) 6(0.22) 6(0.23) 当前吸烟Current smoking 45(1.31) 41(1.33) 39(1.19) 40(1.27) 27(0.94) 32(1.17) 25(0.94) 饮酒状态Drinking status 不饮酒① No drinking ① 3 203(93.06) 2 824(91.63) 3 100(94.51) 2 975(94.68) 2 700(94.41) 2 598(94.82) 2 511(94.47) 偶尔饮酒① Occasional drinking ① 227(6.60) 246(7.98) 172(5.24) 152(4.84) 148(5.17) 128(4.67) 138(5.19) 经常饮酒① Often drinking ① 12(0.35) 12(0.39) 8(0.24) 15(0.48) 12(0.42) 14(0.51) 9(0.34) 缺失人数Missing 0 1 0 5 1 5 7 体育锻炼Physical activity 无① No ① 194(5.65) 550(17.90) 1 014(30.98) 1 003(31.96) 909(31.82) 806(29.50) 855(32.22) 偶尔① Occasional ① 2 901(84.53) 1 941(63.18) 1 833(56.00) 1 786(56.92) 1 649(57.72) 1 619(59.26) 1 521(57.31) 经常① Often ① 337(9.82) 581(18.91) 426(13.02) 349(11.12) 299(10.47) 307(11.24) 278(10.47) 缺失人数Missing 10 11 7 9 4 13 11 高血压Hypertension 无① No ① 2 595(75.48) 2 281(74.03) 2 309(70.40) 2 099(66.72) 1 783(62.83) 1 635(59.67) 1 548(58.33) 有① Yes ① 843(24.52) 800(25.97) 971(29.60) 1 047(33.28) 1 055(37.17) 1 105(40.33) 1 106(41.67) 缺失人数Missing 4 2 0 1 23 5 11 糖尿病Diabetes 无① No ① 3 256(94.73) 2 854(92.66) 3 010(91.80) 2 801(89.20) 2 492(87.81) 2 347(85.84) 2 235(84.69) 有① Yes ① 181(5.27) 226(7.34) 269(8.20) 339(10.80) 346(12.19) 387(14.16) 404(15.31) 缺失人数Missing 5 3 1 7 23 11 26 血脂异常Dyslipidemia 无① No ① 2 554(74.20) 1 921(62.31) 1 985(60.54) 1 690(53.72) 1 446(50.65) 1 324(48.29) 1 144(42.93) 有① Yes ① 888(25.80) 1 162(37.69) 1 294(39.46) 1 456(46.28) 1 409(49.35) 1 418(51.71) 1 521(57.07) 缺失人数Missing 0 0 1 1 6 3 0 BMI/(kg·m-2), x±s 24.61±3.39 24.51±3.32 24.78±3.34 24.82±3.29 24.81±3.21 24.86±3.35 24.84±3.37 肌酐/(μmol·L-1) Creatinine /(μmol·L-1), x±s 78.35±23.19 71.99±20.38 67.36±18.22 64.97±18.68 61.05±28.87 59.36±17.22 59.32±14.63 SUA/(μmol·L-1), x±s 229.89±63.49 239.38±65.97 244.32±64.68 258.78±69.77 271.14±69.75 280.67±71.32 285.03±70.84 注:SUA, 血尿酸。
①以人数(占比%)表示。
Note: SUA, serum uric acid.
① Number of people(proportion%).
下载: 导出CSV
表 3 与绝经相关的各时间分段内SUA的估计年度变化:分段线性混合效应模型的结果
Table 3. Estimated annual changes in SUA within each time segment in relation to final menstrual period: results of piece-wise linear mixed effect models
变量Variable 粗模型Crude model 多变量调整模型② Multivariable adjustment model ② β值value (sx) P值value β值value (sx) P值value 绝经相关时间分段①Menopausal related time segments ① A. < -5年years 3.146(0.427) < 0.001 1.992(0.501) < 0.001 B. -5~ < -2年years 4.362(0.554) < 0.001 3.304(0.617) < 0.001 C. -2~ < 2年years 5.541(0.406) < 0.001 4.597(0.489) < 0.001 D. 2~ < 5年years 4.408(0.523) < 0.001 3.652(0.598) < 0.001 E. ≥5年years 2.564(0.364) < 0.001 1.771(0.448) < 0.001 相邻时间分段比较Comparison of adjacent time segments A与B (A∶B) 0.155 0.134 B与C (B∶C) 0.162 0.137 C与D (C∶D) 0.168 0.268 D与E (D∶E) 0.018 0.020 注:①绝经相关时间分段,负值表示绝经前时间,正值表示绝经后时间; ②调整的变量包括基线文化程度、吸烟状态、时变的年龄、BMI、饮酒状态、体育锻炼、肌酐、高血压、糖尿病、血脂异常。
Note: ① Menopausal related time segments, negative values represent premenopausal time, and positive values represent postmenopausal time; ②The adjusted variables included baseline of education level, smoking status, and time-varying age, BMI, drinking status, physical activity, creatinine, hypertension, diabetes, dyslipidemia.
下载: 导出CSV
-
[1] El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American heart association[J]. Circulation, 2020, 142(25): e506-e532. DOI: 10.1161/CIR.0000000000000912. [2] Lobo RA, Gompel A. Management of menopause: a view towards prevention[J]. Lancet Diabetes Endocrinol, 2022, 10(6): 457-470. DOI: 10.1016/S2213-8587(21)00269-2. [3] Cheng ZY, Zheng TZ, Zhang DS, et al. High-level uric acid in asymptomatic hyperuricemia could be an isolated risk factor of cardio-cerebrovascular diseases: a prospective cohort study[J]. Nutr Metab Cardiovasc Dis, 2021, 31(12): 3415-3425. DOI: 10.1016/j.numecd.2021.08.043. [4] Liu J, Tao LX, Zhao Z, et al. Two-year changes in hyperuricemia and risk of diabetes: a five-year prospective cohort study[J]. J Diabetes Res, 2018, 2018: 6905720. DOI: 10.1155/2018/6905720. [5] Li Y, Shen ZY, Zhu BW, et al. Demographic, regional and temporal trends of hyperuricemia epidemics in mainland China from 2000 to 2019: a systematic review and meta-analysis[J]. Glob Health Action, 2021, 14(1): 1874652. DOI: 10.1080/16549716.2021.1874652. [6] 纪晓菁, 王巍. 女性生殖衰老分期与高尿酸血症的相关性[J]. 中国妇幼保健, 2022, 37(10): 1842-1844. DOI: 10.19829/j.zgfybj.issn.1001-4411.2022.10.029.Ji XJ, Wang W. Correlation between female reproductive aging stages and hyperuricemia[J]. Maternal and Child Health Care of China, 2022, 37(10): 1842-1844. DOI: 10.19829/j.zgfybj.issn.1001-4411.2022.10.029. [7] Cho SK, Winkler CA, Lee SJ, et al. The prevalence of hyperuricemia sharply increases from the late menopausal transition stage in middle-aged women[J]. J Clin Med, 2019, 8(3): 296. DOI: 10.3390/jcm8030296. [8] Hak AE, Choi HK. Menopause, postmenopausal hormone use and serum uric acid levels in US women: the Third National Health and Nutrition Examination Survey[J]. Arthritis Res Ther, 2008, 10(5): R116. DOI: 10.1186/ar2519. [9] Stöckl D, Döring A, Thorand B, et al. Reproductive factors and serum uric acid levels in females from the general population: the KORA F4 study[J]. PLoS One, 2012, 7(3): e32668. DOI: 10.1371/journal.pone.0032668. [10] Koga M, Saito H, Mukai M, et al. Factors contributing to increased serum urate in postmenopausal Japanese females[J]. Climacteric, 2009, 12(2): 146-152. DOI: 10.1080/13697130802607719. [11] Hak AE, Curhan GC, Grodstein F, et al. Menopause, postmenopausal hormone use and risk of incident gout[J]. Ann Rheum Dis, 2010, 69(7): 1305-1309. DOI: 10.1136/ard.2009.109884. [12] Teramura S, Sankai T, Yamagishi K, et al. Changes in cardiovascular disease risk factors during menopausal transition in Japanese women: the Circulatory Risk in Communities Study (CIRCS)[J]. Menopause, 2023, 30(1): 88-94. DOI: 10.1097/GME.0000000000002081. [13] Li WJ, Huang ZG, Fang W, et al. Remnant cholesterol variability and incident ischemic stroke in the general population[J]. Stroke, 2022, 53(6): 1934-1941. DOI: 10.1161/STROKEAHA.121.037756. [14] Dai QY, Wu SL, Cao ZF, et al. Trajectories of lipids around the menopause transition in Chinese women: results of the Kailuan cohort study[J]. Fertil Steril, 2023, 119(6): 1057-1067. DOI: 10.1016/j.fertnstert.2023.02.016. [15] Naumova EN, Must A, Laird NM. Tutorial in Biostatistics: evaluating the impact of 'critical periods' in longitudinal studies of growth using piecewise mixed effects models[J]. Int J Epidemiol, 2001, 30(6): 1332-1341. DOI: 10.1093/ije/30.6.1332. [16] Gong M, Wen S, Nguyen T, et al. Converging relationships of obesity and hyperuricemia with special reference to metabolic disorders and plausible therapeutic implications[J]. Diabetes Metab Syndr Obes, 2020, 13: 943-962. DOI: 10.2147/DMSO.S232377. [17] Li GY, Qian XD, Ma CM, et al. The dose-response relationship between sex hormones and hyperuricemia in different gender: NHANES 2013-2016[J]. Front Endocrinol (Lausanne), 2022, 13: 1035114. DOI: 10.3389/fendo.2022.1035114. [18] Yahyaoui R, Esteva I, Haro-Mora JJ, et al. Effect of long-term administration of cross-sex hormone therapy on serum and urinary uric acid in transsexual persons[J]. J Clin Endocrinol Metab, 2008, 93(6): 2230-2233. DOI: 10.1210/jc.2007-2467. [19] Wang Y, Tang R, Luo M, et al. Follicle stimulating hormone and estradiol trajectories from menopausal transition to late postmenopause in indigenous Chinese women[J]. Climacteric, 2021, 24(1): 80-88. DOI: 10.1080/13697137.2020.1775807. [20] Mumford SL, Dasharathy SS, Pollack AZ, et al. Serum uric acid in relation to endogenous reproductive hormones during the menstrual cycle: findings from the BioCycle study[J]. Hum Reprod, 2013, 28(7): 1853-1862. DOI: 10.1093/humrep/det085. [21] Jung JH, Song GG, Lee YH, et al. Serum uric acid levels and hormone therapy type: a retrospective cohort study of postmenopausal women[J]. Menopause, 2018, 25(1): 77-81. DOI: 10.1097/GME.0000000000000953. [22] Wang HS, Yao J, Ding N, et al. Correlation of uric acid with body mass index based on NHANES 2013-2018 data: a cross-sectional study[J]. Medicine, 2022, 101(39): e30646. DOI: 10.1097/MD.0000000000030646. [23] Bi M, Feng A, Liu YZ, et al. U-shaped association of serum uric acid with cardiovascular disease risk scores and the modifying role of sex among Chinese adults[J]. Nutr Metab Cardiovasc Dis, 2023, 33(5): 1066-1076. DOI: 10.1016/j.numecd.2023.02.025. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 530
- HTML全文浏览量: 237
- PDF下载量: 67
- 被引次数: 0