

Association of multimorbidity patterns with activity of daily living and instrumental activity of daily living disability among ≥45 years middle-aged and elderly population in China
-
摘要:
目的 聚类中国≥45岁中老年人多重慢性病模式的流行情况,并探讨多重慢性病模式与日常生活能力(activity of daily living, ADL)和工具性日常生活能力(instrumental activity of daily living,IADL)残疾的关联性。 方法 基于2018年中国健康与养老追踪调查(China Health and Retirement Longitudinal Study,CHARLS)数据库,以19 745名≥45岁中老年人为研究对象,采用双向聚类法(two-way clustering framework,TCF)识别非随机多重慢性疾病模式后进行人群聚类,并采用logistic回归分析模型分析多重慢性病模式与ADL和IADL残疾的相互关系。 结果 中国中老年人多重慢性病患者例数为10 941,占55.4%,可聚类为心脑血管-代谢模式、呼吸系统-内脏模式和消化-关节-精神模式,根据多重慢性病模式的关联强度将人群划分为5个多重慢性病关联组。其中,高度关联心脑血管-代谢模式和消化-关节-精神模式人群的ADL和IADL残疾负担最重(OR=4.696, 95% CI: 4.196~5.255, P < 0.001; OR=3.155, 95% CI: 2.840~3.504, P < 0.001),高度关联心脑血管-代谢模式合并中度关联呼吸系统-内脏模式的人群罹患ADL和IADL残疾的风险次之(OR=2.821, 95% CI: 2.210~3.602, P < 0.001; OR=2.662, 95% CI: 2.120~3.342, P < 0.001)。 结论 中国中老年人群中高度关联心脑血管-代谢模式发生ADL和IADL残疾的风险最高。 Abstract:Objective To cluster the epidemic situation of multimorbidity patterns in middle-aged and elderly people aged 45 years and above in China, and explore the relationship between multimorbidity patterns and activity of daily living (ADL)/instrumental activity of daily living (IADL) disability. Methods Based on the 2018 China Health and Retirement Longitudinal Study (CHARLS), the study included a total of 19 745 individuals aged 45 years and older from the middle-aged and elderly population. To identify non-random multimorbidity patterns, a two-way clustering framework (TCF) was utilized for clustering people, while logistic regression was employed to analyze the association between multimorbidity patterns and ADL/IADL disability. Results The number of middle-aged and elderly patients with multimorbidity in China was 10 941, accounting for 55.4% of the sample, which could be clustered into three patterns: cardio-cerebrovascular-metabolic pattern, respiratory system-visceral pattern and digestion-articular-mental pattern. According to the association strength of multimorbidity patterns, the population was divided into five multimorbidity association groups. ADL/IADL disability burden was the highest in people with highly related cardio-cerebrovascular-metabolic pattern and digestion-articular-mental pattern (OR=4.696, 95% CI: 4.196-5.255, P < 0.001; OR=3.155, 95% CI: 2.840-3.504, P < 0.001). The risk of ADL /IADL disability in people with highly related cardio-cerebrovascular metabolic pattern and moderate related respiratory system-visceral pattern was the second (OR=2.821, 95% CI: 2.210-3.602, P < 0.001; OR=2.662, 95% CI: 2.120-3.342, P < 0.001). Conclusions The risk of ADL /IADL disability is the highest in middle-aged and elderly people with highly related cardio-cerebrovascular metabolic patterns. -

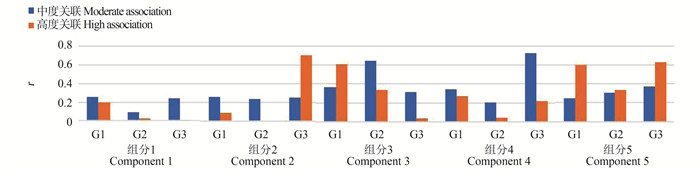
图 1 5类多重慢性病模式特征
G1心脑血管-代谢模式(高血压、血脂异常、糖尿病和血糖升高、心脏病、脑卒中、与记忆相关的疾病);G2呼吸系统-内脏模式(慢性肺部疾病、肝脏疾病、肾脏疾病、哮喘);G3消化-关节-精神模式(胃部疾病或消化系统疾病、情感及精神方面问题、关节炎和风湿病)。
Figure 1. Characteristics of five types of multimorbid
G1 cardio-cerebrovascular-metabolic pattern (hypertension, dyslipidemia, diabetes and high blood sugar, heart disease, stroke, memory-related diseases); G2 respiratory system-visceral pattern (chronic lung disease, liver disease, kidney disease, asthma) and G3 digestion-articular-mental pattern (diseases of the stomach or digestive system, emotional and psychiatric problems, arthritis and rheumatism).
表 1 调查对象基本情况
Table 1. Baseline characteristics of subjects in cross-lagged analysis
变量Variable 总人数① Total ① (n=19 745) ADL残疾① ADL disability ① (n=3 636) 无ADL残疾① No ADL disability ① (n=16 109) IADL残疾① IADL disability ① (n=14 439) 无IADL残疾① No IADL disability ① (n=5 306) 年龄组/岁Age group/years 45~ < 60 8 652(43.8) 794(9.2) 7 858(90.8) 1 262(14.6) 7 390(85.4) 60~ < 75 8 695(44.0) 1 907(21.9) 6 788(78.0) 2 726(31.4) 5 969(68.6) 75~ < 90 2 301(11.7) 875(38.0) 1 426(62.0) 1 237(53.8) 1 064(46.2) ≥90 97(0.5) 60(62.0) 37(38.0) 81(83.5) 16(16.5) 性别Gender 男Male 9 303(47.1) 1 366(37.6) 7 937(49.3) 1 957(21.0) 7 346(79.0) 女Female 10 442(52.9) 2 270(62.4) 8 172(50.7) 3 349(24.3) 7 093(75.7) 教育水平Education level 小学以下Below primary school 8 584(43.5) 2 259(26.0) 6 325(74.0) 3 462(40.3) 5 122(59.7) 小学Primary school 4 348(22.0) 688(15.8) 3 660(84.2) 979(22.5) 3 369(77.5) 中学及以上Secondary school and above 6 813(34.5) 689(10.0) 6 124(90.0) 865(12.7) 5 948(87.3) 居住地区Region 城镇Urban 4 924(24.9) 652(13.2) 4 272(86.8) 898(18.3) 4 026(81.7) 农村Rural 14 735(74.6) 2 977(20.2) 11 758(79.8) 4 399(29.9) 10 336(70.1) 特殊地区Special area 86(0.4) 7(8.1) 79(91.9) 9(10.5) 77(89.5) 婚姻状况Marital status 已婚Married 16 809(85.1) 2 693(16.0) 14 116(84.0) 3 970(23.6) 12 839(76.4) 离异Divorced 312(1.6) 64(20.5) 248(79.5) 76(24.4) 236(75.6) 丧偶或其他Widowed or other 2 624(33.5) 879(24.2) 1 745(66.5) 1 260(48.0) 1 364(52.0) 慢性病数量Number of chronic diseases 0 4 137(21.0) 197(4.8) 3 940(95.2) 490(11.8) 3 647(88.2) 1 4 667(23.6) 516(11.0) 4 151(89.0) 884(18.9) 3 783(81.1) ≥2 10 941(55.4) 2 923(26.7) 8 018(73.3) 3 932(35.9) 7 009(64.1) 注: ADL, 日常生活能力; IADL, 工具性日常生活能力。
①以人数(占比/%)表示。
Note: ADL, activity of daily living; IADL, instrumental activity of daily living.
① Number of people(proportion/%). 下载: 导出CSV
下载: 导出CSV
表 2 分析ADL和IADL残疾与样本特征之间关系的logistic回归分析模型
Table 2. Logistic regression models to analyze the relationship between ADL/ IADL disability and sample characteristics
变量Variable ADL IADL 校正前Before adjustment OR值value (95% CI) 校正后① After adjusting ① OR值value (95% CI) 校正前Before adjustment OR值value (95% CI) 校正后① After adjusting ① OR值value (95% CI) 年龄组/岁Age group/years 60~ < 75 2.780(2.544~3.039) 1.837(1.667~2.023) 2.674(2.481~2.882) 1.749(1.610~1.900) 75~ < 90 6.073(5.432~6.788) 3.612(3.180~4.104) 6.808(6.151~7.534) 4.030(3.588~4.527) ≥90 16.049(10.586~24.332) 10.245(6.518~16.104) 29.645(17.284~50.846) 16.819(9.527~29.691) 性别Gender 女Female 1.614(1.499~1.738) 1.366(1.255~1.488) 1.772(1.661~1.891) 1.437(1.332~1.549) 教育水平Education level 小学Primary school 1.671(1.492~1.871) 1.291(1.142~1.459) 1.998(1.807~2.210) 1.572(1.410~1.753) 小学以下Below primary school 3.174(2.895~3.481) 1.843(1.653~2.056) 4.648(4.276~5.052) 2.816(2.556~3.103) 居住地区Region 农村Rural 1.659(1.514~1.818) 1.580(1.422~1.755) 1.908(1.761~2.068) 1.624(1.478~1.784) 特殊经济地区Special area 0.581(0.267~1.263) 0.574(0.251~1.311) 0.524(0.262~1.049) 0.463(0.218~0.983) 婚姻状况Marital status 离异Divorced 1.353(1.025~1.786) 1.509(1.106~2.058) 1.041(0.802~1.352) 1.184(0.881~1.592) 丧偶或其他Widowed or other 2.640(2.411~2.892) 1.304(1.172~1.452) 2.987(2.745~3.251) 1.394(1.262~1.540) 慢性病数量Number of chronic diseases 1 2.486(2.098~2.946) 2.095(1.741~2.520) 1.739(1.543~1.960) 1.447(1.264~1.656) ≥2 7.291(6.280~8.464) 5.489(4.663~6.462) 4.175(3.770~4.624) 3.182(2.833~3.575) 注: ADL, 日常生活能力; IADL, 工具性日常生活能力。
①代表根据年龄、性别、居住地区、教育程度、婚姻状况和慢性病数量调整的多变量logistic回归模型,P < 0.001。
Note: ADL, activity of daily living; IADL, instrumental activity of daily living.
① Multivariate logistic regression model adjusted for age, gender, region, education level, marital status, and number of chronic diseases, P < 0.001.
下载: 导出CSV
表 3 多重慢性病关联组分与ADL和IADL残疾的logistic回归分析模型
Table 3. Logistic regression analysis of multimorbidity-related components and ADL /IADL disability
多重慢性病组分Multimorbidity component 人数(占比%) Number of people (proportion%) ADL IADL 校正后After adjusting OR值value (95% CI) 校正后After adjusting OR值value (95% CI) 组分1 Component 1 11 079(56.1) 1.000 1.000 组分2 Component 2 1 025(5.2) 2.271(1.901~2.715) 1.708(1.453~2.007) 组分3 Component 3 4 193(21.2) 2.821(2.210~3.602) 2.662(2.120~3.342) 组分4 Component 4 566(2.9) 2.311(2.073~2.577) 1.850(1.681~2.037) 组分5 Component 5 2 882(14.6) 4.696(4.196~5.255) 3.155(2.840~3.504) 注: ADL, 日常生活能力; IADL, 工具性日常生活能力。
Note: ADL, activity of daily living; IADL, instrumental activity of daily living.
下载: 导出CSV
-
[1] 宁吉喆. 第七次全国人口普查主要数据情况[J]. 中国统计, 2021(5): 4-5.Ning JZ. Main data of the seventh national census[J]. China Statistics, 2021(5): 4-5. [2] Kamiya Y, Sim NM, Koshy N, et al. World Population Ageing 2017 Highlights[J]. Statistical Papers-United Nations (Ser. A), Population and Vital Statistics Report, 2018. DOI: 10.18356/10e32e81-en. [3] Yao SS, Cao GY, Han L, et al. Prevalence and patterns of multimorbidity in a nationally representative sample of older Chinese: results from the China health and retirement longitudinal study[J]. J Gerontol A Biol Sci Med Sci, 2020, 75(10): 1974-1980. DOI: 10.1093/gerona/glz185. [4] Palladino R, Lee JT, Ashworth M, et al. Associations between multimorbidity, healthcare utilisation and health status: evidence from 16 European countries[J]. Age Ageing, 2016, 45(3): 431-435. DOI: 10.1093/ageing/afw044. [5] Kirchberger I, Meisinger C, Heier M, et al. Patterns of multimorbidity in the aged population. Results from the KORA-Age study[J]. PLoS One, 2012, 7(1): e30556. DOI: 10.1371/journal.pone.0030556. [6] Zhou JY, Wei MY, Zhang JY, et al. Association of multimorbidity patterns with incident disability and recovery of independence among middle-aged and older adults[J]. Age Ageing, 2022, 51(8): afac177. DOI: 10.1093/ageing/afac177. [7] Tas U, Verhagen AP, Bierma-Zeinstra SM, et al. Prognostic factors of disability in older people: a systematic review[J]. Br J Gen Pract, 2007, 57(537): 319-323. [8] Luo YN, Su BB, Zheng XY. Trends and challenges for population and health during population aging - China, 2015-2050[J]. China CDC Wkly, 2021, 3(28): 593-598. DOI: 10.46234/ccdcw2021.158. [9] Wikström K, Lindström J, Harald K, et al. Clinical and lifestyle-related risk factors for incident multimorbidity: 10-year follow-up of Finnish population-based cohorts 1982-2012[J]. Eur J Intern Med, 2015, 26(3): 211-216. DOI: 10.1016/j.ejim.2015.02.012. [10] 陆姣, 王媛, 袁媛. 慢性病疾病组合模式识别方法的应用与比较[J]. 中国卫生统计, 2022, 39(3): 477-480. DOI: 10.3969/j.issn.1002-3674.2022.03.038.Lu J, Wang Y, Yuan Y. Application and comparison of combined pattern recognition methods for chronic diseases[J]. China Journal of Health Statistics, 2022, 39(3): 477-480. DOI: 10.3969/j.issn.1002-3674.2022.03.038. [11] Hu XL, Huang J, Lyu YQ, et al. Status of prevalence study on multimorbidity of chronic disease in China: systematic review[J]. Geriatr Gerontol Int, 2015, 15(1): 1-10. DOI: 10.1111/ggi.12340. [12] Wang ZJ, Peng WJ, Li MY, et al. Association between multimorbidity patterns and disability among older people covered by long-term care insurance in Shanghai, China[J]. BMC Public Health, 2021, 21(1): 418. DOI: 10.1186/s12889-021-10463-y. [13] Marengoni A, Roso-Llorach A, Vetrano DL, et al. Patterns of multimorbidity in a population-based cohort of older people: sociodemographic, lifestyle, clinical, and functional differences[J]. J Gerontol A Biol Sci Med Sci, 2020, 75(4): 798-805. DOI: 10.1093/gerona/glz137. [14] 王亚林, 张静, 朱慕云. 血清标志物在老年慢性阻塞性肺疾病并发肌少症中的作用[J]. 临床肺科杂志, 2022, 27(8): 1243-1248. DOI: 10.3969/j.issn.1009-6663.2022.08.023.Wang YL, Zhang J, Zhu MY. The role of serum markers in elderly patients with chronic obstructive pulmonary disease complicated with sarcopenia[J]. J Clin Pulm Med, 2022, 27(8): 1243-1248. DOI: 10.3969/j.issn.1009-6663.2022.08.023. [15] 罗宇, 周平. 肌肉减少症与骨关节炎之间的联系及共同发病机制[J]. 现代医学与健康研究电子杂志, 2020, 4(24): 107-111. DOI: 2096-3718.2020.24.0107.05.Luo Y, Zhou P. Association and common pathogenesis between sarcopenia and osteoarthritis[J]. Mod Med Health Res Electron J, 2020, 4(24): 107-111. DOI: 2096-3718.2020.24.0107.05. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 630
- HTML全文浏览量: 199
- PDF下载量: 66
- 被引次数: 0