

Epidemiological characteristics and spatial-temporal clustering of scarlet fever in Hangzhou from 2010 to 2023
-
摘要:
目的 探索2010―2023年杭州市猩红热的流行病学特征及其时空分布特点,为杭州市猩红热防控策略的制定和合理配置卫生资源提供科学依据。 方法 2010―2023年杭州市猩红热发病数据来源于中国疾病预防控制信息系统,采用Joinpoint5.1.0软件对猩红热发病数据进行趋势分析,运用ArcGIS 10.8软件开展空间自相关分析,使用SaTScan 10.1.2软件进行时空扫描分析。 结果 2010―2023年杭州市猩红热的年均发病率为5.06/10万;Joinpoint回归分析结果显示,2015―2023年杭州市各年的猩红热发病率呈下降趋势。病例分布呈季节性,春末夏初(4―6月)和秋末冬初(11月―次年1月)为发病高峰期。病例主要为3~<9岁组(85.79%)、男性(61.00%)和幼托儿童(47.09%)。拱墅区和上城区是杭州市猩红热的高发区域,占所有报告病例的35.73%(2 459/6 882)。全局自相关分析显示,除2011年、2013年和2014年外,其余各年猩红热发病率均存在空间相关性(均P<0.05);局部空间自相关分析显示,2010―2023年杭州市猩红热发病率均有热点区域(“高-高”聚集)出现,且相对集中分布于东北部和中部区域。时空扫描分析共探测到3个聚集区,其中一类聚集区主要位于上城区、拱墅区的13个街道,聚集时间为2014年3月―2016年6月。 结论 2010―2023年,杭州市猩红热疫情先呈上升趋势,自2015年后呈下降趋势,全市存在时空聚集性,主要集中于杭州市东北部和中部区域,应加强高发地区和人群的健康教育以及疾病监测工作。 Abstract:Objective This study aims to explore the epidemiology and spatial-temporal clustering characteristics of scarlet fever in Hangzhou from 2010 to 2023, providing a scientific basis for the formulation of prevention and control strategies for scarlet fever as well as the rational allocation of health resources in Hangzhou. Methods The incidence data of scarlet fever in Hangzhou from 2010 to 2023 came from China Disease Prevention and Control Information System. Joinpoint 5.1.0 software was used to analyze the trend of scarlet fever incidence data, and ArcGIS 10.8 software was used to carry out spatial autocorrelation analysis. SaTScan 10.1.2 was used to perform spatio-temporal scan analysis. Results The average annual incidence of scarlet fever in Hangzhou from 2010 to 2023 was 5.06 per 100 000 population. Joinpoint regression analysis revealed a decreasing trend in the incidence of scarlet fever in Hangzhou from 2015 to 2023. The distribution of cases exhibited distinct seasonal patterns, peaking in late spring to early summer (April to June) and late autumn to early winter (November to January of the following year). The majority of cases were among children aged 3~9 years (85.79%), males (61.00%), and preschool children (47.09%). Gongshu District and Shangcheng District were identified as high-incidence areas, accounting for 35.73% (2 459/6 882) of all reported cases. The global autocorrelation analysis showed that the incidence of scarlet fever was spatially correlated in all years except 2011, 2013 and 2014 (P<0.05). Local spatial autocorrelation analysis indicated the presence of hotspots ("high-high" clusters) of scarlet fever incidence in Hangzhou from 2010 to 2023, relatively concentrated in the northeastern and central regions. Spatiotemporal scan analysis detected three clusters, of which the primary cluster encompassed 13 neighborhoods in Shangcheng and Gongshu Districts, spanning from March 2014 to June 2016. Conclusions From 2010 to 2023, the epidemic of scarlet fever in Hangzhou initially shows a fluctuating upward trend, followed by a fluctuating downward trend after 2015. There is a significant spatial-temporal clustering in the city, primarily concentrated in the northeastern and central regions of Hangzhou. Enhanced health education and disease surveillance efforts should be implemented in high-incidence areas and populations. -

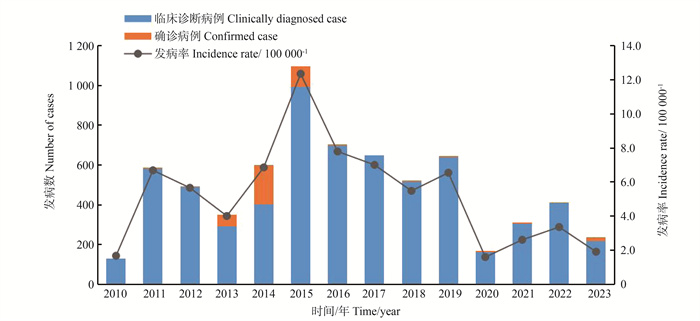
图 1 2010―2023年杭州市猩红热报告病例数及发病率
Figure 1. Number of cases and incidence of scarlet fever in Hangzhou, 2010-2023

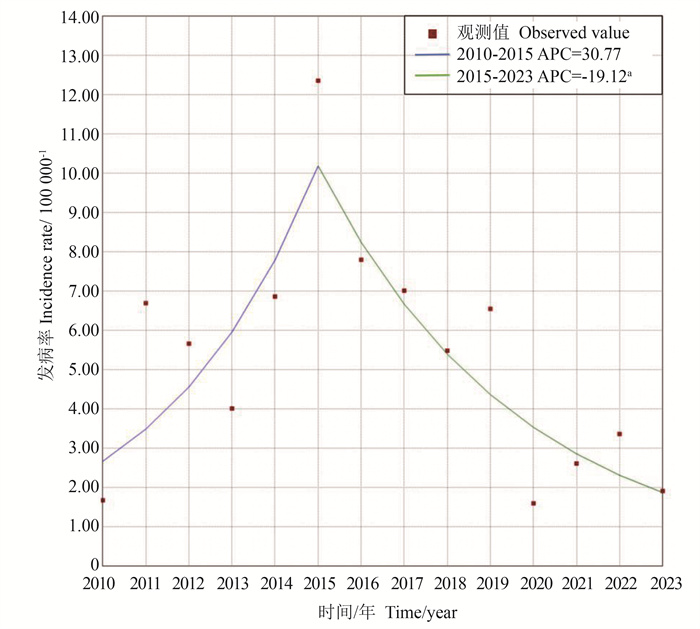
图 2 2010―2023年杭州市猩红热发病率变化趋势Jointpoint回归分析
APC:年度变化百分比;a: P<0.05。
Figure 2. Jointpoint regression analysis of scarlet fever incidence in Hangzhou from 2010 to 2023
annual percent change; a: P<0.05.

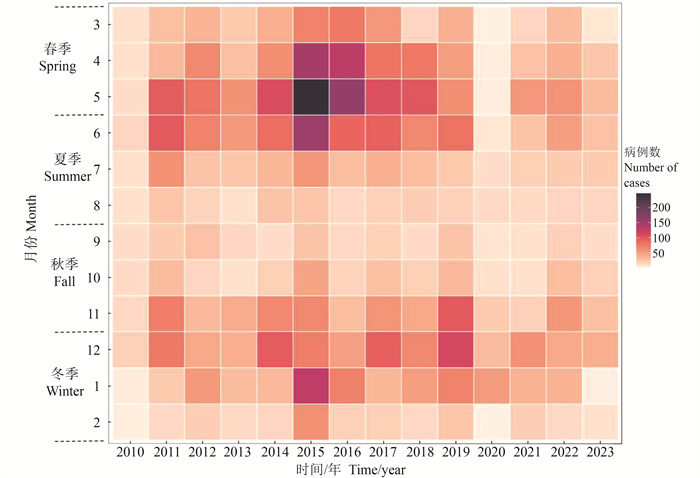
图 3 2010―2023年杭州市猩红热病例发病时间分布
Figure 3. Time distribution of scarlet fever cases in Hangzhou from 2010 to 2023
表 1 2010―2023年杭州市猩红热发病率全局空间自相关分析
Table 1. Global spatial autocorrelation analysis of incidence of scarlet fever in Hangzhou from 2010 to 2023
年份 Year Moran′s I Z 值 value P 值 value 2010 0.12 2.06 0.039 2011 0.01 1.11 0.266 2012 0.05 2.40 0.016 2013 0.06 1.94 0.053 2014 0.03 1.59 0.111 2015 0.05 3.22 0.001 2016 0.19 6.07 <0.001 2017 0.17 6.48 <0.001 2018 0.11 3.23 0.001 2019 0.07 3.58 <0.001 2020 0.19 3.87 <0.001 2021 0.50 10.68 <0.001 2022 0.33 14.88 <0.001 2023 0.48 9.45 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 2010―2023年杭州市猩红热病例时空扫描结果
Table 2. Spatial-temporal scan results of scarlet fever cases in Hangzhou from 2010 to 2023
聚集区类型
Type of clusters实际病例数
Number of actual cases期望病例数
Number of expected cases半径
Radiu/km聚集时间/年-月
Cluster time/year-month涉及街道(乡镇)数量
Number of towns and streets involvedRR 值value LLR 值value P 值 value 一类聚集区 Class one clusters 739 129 6.28 2014.03―2016.06 13 6.28 706.38 <0.001 二类聚集区1 Class two clusters 1 168 18 13.65 2021.05―2022.07 9 9.29 222.93 <0.001 二类聚集区2 Class two clusters 2 209 70 22.69 2015.01―2015.06 38 3.01 89.46 <0.001
下载: 导出CSV
-
[1] Ma YX, Gao SS, Kang Z, et al. Epidemiological trend in scarlet fever incidence in China during the COVID-19 pandemic: a time series analysis [J]. Front Public Health, 2022,10:923318. DOI: 10.3389/fpubh.2022.923318. [2] Johnson AF, LaRock CN. Antibiotic treatment, mechanisms for failure, and adjunctive therapies for infections by group A streptococcus [J]. Front Microbiol. 2021, 4(12): 760255. DOI: 10.3389/fmicb.2021.760255. [3] Pardo S, Perera TB. Scarlet Fever, 2023. In: StatPearls[Internet]. treasure Island(FL): StatPearls Publishing. [4] 向媛媛. 全国猩红热发病空间分布特征及贝叶斯时空建模研究[D]. 兰州: 兰州大学, 2024.Xiang YY. Spatial distribution characteristics of scarlet fever in China and Bayesian spatio-temporal modeling [D]. Lanzhou: Lanzhou University, 2024. [5] Lu QB, Wu HC, Ding ZY, et al. Analysis of epidemiological characteristics of scarlet fever in Zhejiang Province, China, 2004-2018 [J]. Int J Environ Res Public Health, 2019, 16(18): 3454. DOI: 10.3390/ijerph16183454. [6] 中华人民共和国卫生部. 猩红热诊断标准: WS 282—2008 [S]. 北京: 人民卫生出版社, 2008: 2.Ministry of Health of the People′s Republic of China. Diagnostic criteria for scarlet fever: WS 282-2008 [S]. Beijing: People′s Medical Publishing House, 2008: 2. [7] Rao HX, Li DM, Zhao XY, et al. Spatiotemporal clustering and meteorological factors affected scarlet fever incidence in mainland China from 2004 to 2017 [J]. Sci Total Environ, 2021, 777: 146145. DOI: 10.1016/j.scitotenv. [8] Liu YH, Chan TC, Yap LW, et al. Resurgence of scarlet fever in China: a 13-year population-based surveillance study [J]. Lancet Infect Dis, 2018, 18(8): 903-912. DOI: 10.1016/S1473-3099(18)30231-7. [9] Ma YX, Gao SS, Kang Z, et al. Epidemiological trend in scarlet fever incidence in China during the COVID-19 pandemic: a time series analysis [J]. Front Public Health, 2022, 10: 923318. DOI: 10.3389/fpubh.2022.923318. [10] Song SS, Wang P, Li J, et al. The indirect impact of control measures in COVID-19 pandemic on the incidence of other infectious diseases in China [J]. Public Health Pract, 2022, 4: 100278. DOI: 10.1016/j.puhip.2022.100278. [11] 高桂玲, 钱婧娴, 姚霞菁, 等. 2017-2021年上海市松江区猩红热流行病学特征分析[J]. 华南预防医学, 2023, 49(6): 747-750. DOI: 10.12183/j.scjpm.2023.0747.Gao GL, Qian JX, Yao XJ, et al. Epidemiological characteristics of scarlet fever in Songjiang district, Shanghai, 2017-2021 [J]. South China Prev Med, 2019, 49(6): 747-750. DOI: 10.12183/j.scjpm.2023.0747. [12] 何飞, 张雅婷, 朱兵清, 等. 2009-2018年湖北省猩红热流行病学特征分析[J]. 中华预防医学杂志, 2020, 54(5): 568-571. DOI: 10.3760/cma.j.cn112150-20190509-00378.He F, Zhang YT, Zhu BQ, et al. Epidemiological characteristics of scarlet fever in Hubei Province from 2009 to 2018 [J]. Chin J Prev Med, 2020, 54(5): 568-571. DOI: 10.3760/cma.j.cn112150-20190509-00378. [13] 马涛, 洪镭, 杜雪飞, 等. 2014-2019年南京市猩红热流行特征和时空聚集性[J]. 中华疾病控制杂志, 2021, 25(3): 346-351. DOI: 10.16462/j.cnki.zhjbkz.2021.03.018.Ma T, Hong L, Du XF, et al. Epidemiological characteristics and temporal-spatial clustering of scarlet fever in Nanjing from 2014 to 2019 [J]. Chin J Dis Control Prev, 2021, 25(3): 346-351. DOI: 10.16462/j.cnki.zhjbkz.2021.03.018. [14] Cui JY, Zhang YW, Ge H, et al. Patterns in the incidence of scarlet fever among children aged 0-9 years - China, 2010-2019 [J]. China CDC Wkly, 2023, 5(34): 756-762. DOI: 10.46234/ccdcw2023.143. [15] Li C, Liao RJ, Zhu WH, et al. Spatiotemporal dynamics and potential ecological drivers of acute respiratory infectious diseases: an example of scarlet fever in Sichuan Province [J]. BMC Public Health, 2022, 22(1): 2139. DOI: 10.1186/s12889-022-14469-y. [16] Buckee C, Noor A, Sattenspiel L. Thinking clearly about social aspects of infectious disease transmission [J]. Nature, 2021, 595(7866): 205-213. DOI: 10.1038/s41586-021-03694-x. [17] Yang SQ, Fang ZG, Lv CX, et al. Spatiotemporal cluster analysis of COVID-19 and its relationship with environmental factors at the city level in mainland China [J]. Environ Sci Pollut Res Int, 2022, 29(9): 13386-13395. DOI: 10.1007/s11356-021-16600-9. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 255
- HTML全文浏览量: 67
- PDF下载量: 36
- 被引次数: 0