

Analysis of the prevalence trend of drug resistance among high risk population of multi drug resistant-tuberculosis in Wuhan from 2007 to 2020
-
摘要:
目的 回顾性分析2007—2020年武汉市耐药肺结核高危人群耐药流行趋势。 方法 对2007年1月1日—2020年12月31日武汉市新登记的5 139例耐药肺结核高危人群进行筛查, 采用描述性研究、趋势χ2检验和多因素非条件logistic回归分析模型进行统计分析。 结果 武汉市耐药肺结核高危人群结核分枝杆菌总耐药率为35.51%(1 600/4 506),6种抗结核药物的任何耐药频度依次为:异烟肼(isoniazid,H)>利福平(rifampin,R)>链霉素(streptomycin,S)>氧氟沙星(ofloxacin,O)>乙胺丁醇(ethambutol,E)>卡那霉素(Kanamycin,K)。2007—2020年除O耐药率外,总耐药率、耐多药率和H、R、S、E、K耐药率均呈上升趋势(R耐药率:P=0.002,其余均有P < 0.001)。2015—2020年耐药、耐多药、H、E、S、O、K耐药率均无上升趋势,R耐药率呈上升趋势(P=0.002)。 结论 2007—2020年武汉市耐药肺结核高危人群耐药疫情呈上升趋势。虽然2015—2020年未呈上升趋势,但仍迫切需要加强对此类人群的管理和控制。 Abstract:Objective To retrospectively analyze the drug resistance prevalence trend of drug resistance-tuberculosis(DR-TB) high-risk populations in Wuhan from 2007 to 2020. Methods From January 1, 2007 to December 31, 2020, a total of 5 139 at risk individuals of DR-TB newly registered in Wuhan were screened. By carrying out a descriptive study, χ2 test and multivariate unconditional logistic regression, the prevalence trend and influencing factors of drug resistance were analyzed. Results The overall drug resistance rate among these individuals was 35.51% (1 600/4 506). The ranking of resistance rates of six different anti-TB drugs was as following, Isoniazid (H)>Rifampin (R)>Streptomycin (S)>Ofloxacin (O)>ethambutol (E)>Kanamycin (K). From 2007 to 2020, except the O resistance rate, the overall drug resistance rate, multidrug resistance rate, drug resistance rates of H, R, E, S and K showed an upward trend (R resistance rate: P=0.002, all the others have P < 0.001). From 2015 to 2020, except an upward trend was observed in R resistance rate (P=0.002), the overall drug resistance rate, multidrug resistance rate and drug resistance rates of H, E, S, O and K remained stable. Conclusions From 2007 to 2020, an upward trend of drug resistance among Wuhan's DR-TB at risk populations was observed. Although no upward trend was observed in the period between 2015 and 2020, further strengthening of management and control of such groups is still urgently needed. -
Key words:
- Mycobacterium /
- Tuberculosis /
- Drug resistance /
- Trend /
- Influential factors
-

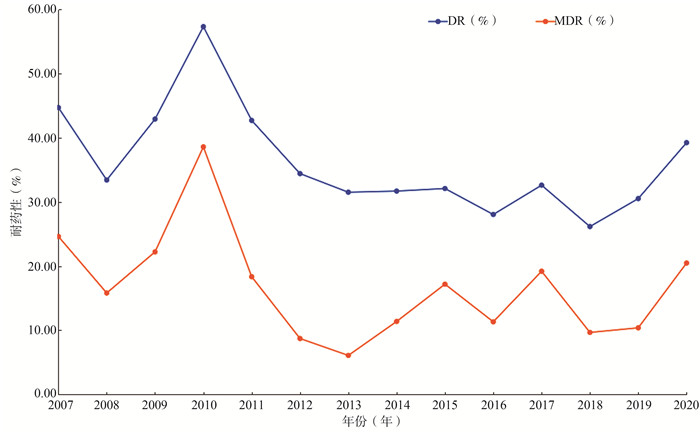
图 1 2007—2020年武汉市耐药高危人群耐药率和耐多药率
Figure 1. Drug resistance rate and multidrug resistance rate of high-risk population in Wuhan from 2007 to 2020

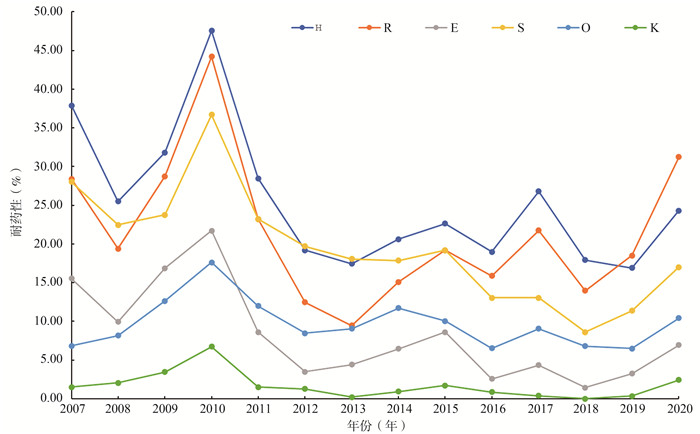
图 2 2007—2020年武汉市耐药高危人群H、R、E、S、O、K耐药率
Figure 2. The drug resistance for H、R、E、S、O and K in high-risk population in Wuhan from 2007 to 2020
表 1 2007—2020年武汉市耐药高危人群耐药筛查率[n(%)]
Table 1. Drug resistance screening rate of high-risk population in Wuhan from 2007 to 2020 [n(%)]
年份(年) 应筛查人数a(例) 实际筛查人数(例) 筛查率(%) 年份(年) 应筛查人数a(例) 实际筛查人数(例) 筛查率(%) 2007 280 264 94.3 2015 387 349 90.2 2008 412 392 95.1 2016 370 353 95.4 2009 273 261 95.6 2017 288 276 95.8 2010 282 267 94.7 2018 291 279 95.9 2011 290 267 92.1 2019 323 308 95.4 2012 445 401 90.1 2020 292 288 98.6 2013 521 476 91.4 2014 356 325 91.3 注:a除培养阴性和污染的菌株数。  下载: 导出CSV
下载: 导出CSV
表 2 4 506株结核分枝杆菌菌株对各种抗结核药物的耐药情况[n(%)]
Table 2. Drug resistance of 4 506 Mycobacterium tuberculosis strains to various anti TB drugs [n(%)]
药敏试验结果 菌株数(例) 率(%) 药敏试验结果 菌株数(例) 率(%) 全敏感 2 906 64.49 耐3种药物 耐≥1种药物a 1 600 35.51 HRS 184 4.08 任何耐H 1 105 24.52 HRO 38 0.84 任何耐R 919 20.40 HRE 35 0.78 任何耐S 864 19.17 HSO 21 0.47 任何耐O 429 9.52 HES 14 0.31 任何耐E 346 7.68 RES 12 0.27 任何耐K 70 1.55 HEO 7 0.16 耐1种药物 RSO 5 0.11 H 161 3.57 HRK 2 0.04 R 150 3.33 ESO 1 0.02 S 136 3.02 HSK 1 0.02 O 108 2.40 REO 1 0.02 E 3 0.07 耐4种药物 K 3 0.07 HRES 102 2.26 耐2种药物 HRSO 47 1.04 HR 160 3.55 HREO 20 0.44 HS 157 3.48 HESO 7 0.16 RS 24 0.53 ESOK 2 0.04 RO 18 0.40 HROK 2 0.04 SO 16 0.36 RESO 2 0.04 HO 13 0.29 HRSK 1 0.02 HE 11 0.24 RESK 1 0.02 RE 11 0.24 耐5种药物 ES 2 0.04 HRESO 67 1.49 EO 1 0.02 HRESK 5 0.11 HK 1 0.02 HRSOK 5 0.11 OK 1 0.02 HREOK 4 0.09 HESOK 1 0.02 注:a 6种抗结核药物中任何耐其中1种药物,其他5种药物是否耐药不做考虑。
下载: 导出CSV
表 3 不同耐药类型2007—2020年耐药χ2趋势分析
Table 3. Analysis of drug resistance χ2 trend of different drug resistance types from 2007 to 2020
耐药类型 2007-2014年 2015-2020年 2007-2020年 χ趋势2值 P值 χ趋势2值 P值 χ趋势2值 P值 耐药 15.69 < 0.001 2.52 0.113 30.21 < 0.001 耐多药 61.73 < 0.001 0.03 0.866 25.47 < 0.001 任何耐H 47.43 < 0.001 0.13 0.724 49.46 < 0.001 任何耐R 57.53 < 0.001 9.51 0.002 10.04 0.002 任何耐E 45.93 < 0.001 1.25 0.264 84.58 < 0.001 任何耐S 15.81 < 0.001 2.07 0.150 75.09 < 0.001 任何耐O 0.49 0.485 0.01 0.919 3.30 0.069 任何耐K 7.94 0.005 0.02 0.878 13.18 < 0.001 注:因2015年武汉市全面推广分子生物学检测方法,以2015年为分界点,分别对2007—2014年和2015—2020年进行趋势χ2检验。
下载: 导出CSV
表 4 不同耐药类型2007—2020年耐药χ2趋势分析
Table 4. Analysis of drug resistance χ2 trend of different drug resistance types from 2007 to 2020
变量 总例数 耐药 耐多药 例数(%) OR(95% CI)值 P值 例数(%) OR(95% CI)值 P值 性别 男 3 692 1 311(35.51) 1.000 564(15.28) 1.000 女 814 289(35.5) 0.977(0.834~1.145) 0.777 145(17.81) 1.202(0.983~1.469) 0.072 年龄(岁) < 25 112 49(43.75) 2.036(1.376~3.014) < 0.001 31(27.68) 4.262(2.697~6.735) < 0.001 25~ < 45 793 328(41.36) 1.847(1.534~2.223) < 0.001 185(23.33) 3.389(2.625~4.374) < 0.001 45~ < 65 2 266 854(37.69) 1.583(1.367~1.834) < 0.001 383(16.90) 2.265(1.811~2.834) < 0.001 ≥65 1 335 369(27.64) 1.000 110(8.24) 1.000 职业 离退人员 1 240 393(31.69) 1.000 160(12.90) 1.000 工人 386 147(38.08) 1.583(1.045~1.681) 0.020 69(17.88) 1.469(1.079~2.001) 0.014 农民/民工 753 260(34.53) 1.137(0.938~1.377) 0.191 121(16.07) 1.292(1.001~1.669) 0.049 商业服务人员 1 626 586(36.04) 1.214(1.038~1.420) 0.015 257(15.81) 1.267(1.024~1.568) 0.029 干部职员 115 38(33.04) 1.064(0.708~1.597) 0.766 19(16.52) 1.336(0.795~2.246) 0.273 其他a 386 176(45.59 1.806(1.430~2.281) < 0.001 83(21.50) 1.849(1.378~2.481) < 0.001 居住地 主城区 2 947 1 050(35.63) 1.000 462(15.68) 1.000 远城区 1 559 550(35.28) 0.985(0.866~1.120) 0.815 247(15.84) 1.013(0.856~1.198) 0.884 登记分类 2或3月末痰涂片阳性 96 25(26.04) 1.000 11(11.46) 1.000 复发/返回 2 807 967(34.45) 1.493(0.940~2.370) 0.088 400(14.25) 1.284(0.679~2.428) 0.440 慢性排菌/复治失败 1 392 509(36.57) 1.637(1.025~2.616) 0.038 232(16.67) 1.545(0.812~2.942) 0.182 初治失败 129 61(47.29) 2.548(1.438~4.514) 0.001 41(31.78) 3.601(1.736~7.465) < 0.001 密切接触MDR-TB涂阳 82 38(46.34) 2.453(1.307~4.603) 0.005 25(30.49) 3.389(1.547~7.427) 0.002 注:a其他职业指除离退人员、工人、农民/民工、商业服务人员和干部职员以外的待业、学生和其他无法界定的职业。
下载: 导出CSV
表 5 武汉市耐药肺结核高危人群耐药和耐多药结核病多因素logistic回归分析
Table 5. The multivariate logistic regression analysis of drug resistance and MDR-TB in high-risk drug-resistant TB patients in Wuhan
变量 耐药 耐多药 OR(95% CI)值 P值 OR(95% CI)值 P值 年龄(岁) < 25 vs. ≥65 1.928(1.299~2.863) 0.001 3.812(2.395~6.065) < 0.001 25~ < 45 vs. ≥65 1.817(1.509~2.189) < 0.001 3.274(2.534~4.231) < 0.001 45~ < 65 vs. ≥65 1.573(1.358~1.823) < 0.001 2.241(1.790~2.805) < 0.001 登记分类 复发/返回vs. 2或3月末痰涂片阳性 1.495(0.939~2.380) 0.091 1.296(0.682~2.466) 0.429 慢性排菌/复治失败vs. 2或3月末痰涂片阳性 1.636(1.021~2.620) 0.041 1.556(0.831~2.980) 0.182 初治失败vs. 2或3月末痰涂片阳性 2.378(1.337~4.230) 0.003 3.209(1.534~6.712) 0.002 密切接触MDR-TB涂阳vs. 2或3月末痰涂片阳性 2.296(1.218~4.326) 0.010 3.002(1.356~6.647) 0.007
下载: 导出CSV
-
[1] WHO. Global tuberculosis report 2021[EB/OL]. (2021-10-14)[2022-03-01]. https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2021. [2] 中国全球基金结核病项目办公室. 中国全球基金结核病项目(一期)实施细则耐多药结核病防治领域[M]. 北京: 北京大学医学出版社, 2010: 31-39.China Global Fund TB Project Office. Implementation details of China Global Fund Tuberculosis Project (phase I)[M]. Beijing: Peking University Medical Press, 2010: 31-39. [3] 唐神结, 许绍发, 李亮. 耐药结核病学[M]. 北京: 人民卫生出版社, 2014: 321-324.Tang SJ, Xu SF, Li L. Drug-Resistant Tuberculosis[M]. Beijing: People's Medical Publishing House, 2014: 321-324. [4] 赵亚玲, 黎舒, 邱媛. 2012-2016年南宁市耐多药肺结核高危人群筛查情况分析[J]. 应用预防医学, 2019, 25(1): 14-17. https://www.cnki.com.cn/Article/CJFDTOTAL-GXYX201901004.htmZhao YL, Li S, Qiu Y. Screening of multi-drug resistance pulmonary tuberculosis in hi-gh-risk group, Nanning, 2012-2016[J]. Applied Prev Med, 2019, 25(1): 14-17. https://www.cnki.com.cn/Article/CJFDTOTAL-GXYX201901004.htm [5] 李佳, 黄玲, 赵玉杭, 等. 福州市2016-2020年耐药肺结核发现情况分析[J]. 中国热带医学, 2021, 21(8): 795-799. DOI: 10.13604/j.cnki.46-1064/r.2021.08.16.Li J, Huang L, Zhao YH, et al. Analysis of drug-resistant pulmonary tuberculosis in Fu-zhou 2016-2020[J]. Chin Trop Med, 2021, 21(8): 795-799. DOI: 10.13604/j.cnki.46-1064/r.2021.08.16. [6] 王坚杰, 周美兰, 段琼红, 等. 2010年湖北省武汉市第5次结核病流行病学抽样调查分析[J]. 中华疾病控制杂志, 2014, 18(4): 326-329. http://zhjbkz.ahmu.edu.cn/article/id/JBKZ201404014Wang JJ, Zhou ML, Duan QH, et al. The fifth tuberculosis epidemiological survey of Wuhan City in 2010[J]. Chin J Dis Control Prev, 2014, 18(4): 326-329. http://zhjbkz.ahmu.edu.cn/article/id/JBKZ201404014 [7] 李永文, 李新旭, 耿红, 等. 山东省结核分枝杆菌的耐药流行状况[J]. 中华结核和呼吸杂志, 2013, 36(9): 667-670. DOI: 10.3760/cma.j.issn.1001-0939.2013.09.007.Li YW, Li XX, Gen H, et al. Epidemic status of drug-resistant Mycobacterium tubercul-osis in Shandong Province, China[J]. Chin J Tuberc Respir Dis, 2013, 36(9): 667-670. DOI: 10.3760/cma.j.issn.1001-0939.2013.09.007. [8] 中华人民共和国卫生部. 全国结核病耐药性基线调查报告(2007-2008年)[M]. 北京: 人民卫生出版社, 2010: 33.Ministry of Health, PRC. National baseline survey of tuberculosis drug resistance (2007-2008)[M]. Beijing: People's Medical Publishing House, 2010: 33. [9] 许可, 丁松宁, 杨晨, 等. 使用倾向得分匹配法评估南京市耐多药结核病的影响因素[J]. 中华疾病控制杂志, 2022, 26(3): 285-289. DOI: 10.16462/j.cnki.zhjbkz.2022.03.008.Xu K, Ding SN, Yang C, et al. Evaluating the influential factors of multidrug-resistant t-uberculosis using a propensity score matching method[J]. Chin J Dis Control Prev, 2022, 26(3): 285-289. DOI: 10.16462/j.cnki.zhjbkz.2022.03.008. [10] Lee EG, Min J, Kang JY, et al. Age-stratified anti-tuberculosis drug resistance profiles i-n South Korea: a multicenter retrospective study[J]. BMC Infect Dis. 2020, 23(1): 446-455. DOI: 10.1186/s12879-020-05157-6. [11] 李君, 朱小梅, 毛玲琼, 等. 温州市2014-2015年耐多药肺结核高危人群筛查情况分析[J]. 中国公共卫生管理, 2017, 33(3): 345-347. DOI: 10.19568/j.cnki.23-1318.2017.03.017.Li J, Zhu XM, Mao LQ, et al. Screening of multi-drug resistance pulmonary tubercu-losis in high-risk group, Wenzhou, 2014-2015[J]. Chin J of PHM, 2017, 33(3): 345-347. DOI: 10.19568/j.cnki.23-1318.2017.03.017. [12] 王坚杰, 周美兰, 杜义祥, 等. 武汉市耐药/耐多药结核病影响因素分析[J]. 中华疾病控制杂志, 2017, 21(2): 164-167. DOI: 10.16462/j.cnki.zhjbkz.2017.02.014.Wang JJ, Zhou ML, Du YX, et al. Analysis on the influential factors of drug resistance and multidrug resistant tuberculosis in Wuhan City[J]. Chin J Dis Control Prev, 2017, 21(2): 164-167. DOI: 10.16462/j.cnki.zhjbkz.2017.02.014. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 580
- HTML全文浏览量: 241
- PDF下载量: 32
- 被引次数: 0