

Analysis and prediction of the epidemiological characteristics of hepatitis A in Hubei Province from 2004 to 2019
-
摘要:
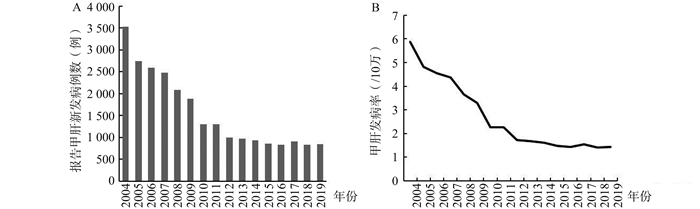
目的 分析湖北省2004―2019年甲型病毒性肝炎(简称“甲肝”)流行病学特征,为评价和制定甲肝防控策略提供科学依据。 方法 采用描述流行病学方法,对湖北省2004―2019年甲肝疫情资料进行统计分析。采用自回归整合移动平均模型(auto regression integrated moving average,ARIMA)季节模型对未来甲肝发病情况进行预测。 结果 湖北省2004―2019年累计报告甲肝病例25 080例,年平均发病率为2.71/10万。甲肝的发病率从2004年的5.88/10万降低到2019年的1.43/10万。发病人群以农民为主(占59.13%)。发病人数构成较高的年龄段主要为35~65岁以下壮年人群(占56.80%)。男女比例为2.03:1,性别比在2019年已经降至1.06。病例主要以散发为主,研究期间共有6次暴发,均与教育机构有关。2010年至2017年间,湖北省儿童的甲肝疫苗接种率均在90%以上。ARIMA模型预测甲肝发病人数会持续下降,在2030年降低到484例,预估发病率低于1/10万。 结论 2004―2019年间,甲肝防控措施成效明显。今后在做好适龄儿童免疫接种工作的同时,需要加强农村人群,尤其是壮年农民的综合防控措施。虽然在2030年还不能消除甲肝发病,但可进一步降低疾病危害。 Abstract:Objective To analyze the epidemiological characteristics of hepatitis A in Hubei Province from 2004 to 2019, so as to provide scientific evidence for the evaluation and formulation of hepatitis A prevention and control strategies. Methods A descriptive epidemiological study was conducted to analyze the data of hepatitis A in Hubei Province from 2004 to 2019. Auto regression integrated moving (ARIMA) average seasonal model was used to predict the occurrence of hepatitis A in the future. Results A total of 25 080 cases of hepatitis A were reported in Hubei Province from 2004 to 2019, and the average annual incidence rate was 2.71/100 000. The incidence rate of hepatitis A dropped from 5.88/100 000 in 2004 to 1.43/100 000 in 2019. The majority of patients were farmers (59.13%). The age of onset was mainly 35-65 years old (56.80%). The ratio of male to female was 2.03:1 in 2014, and decreased to 1.06:1 in 2019. The reported cases were mainly sporadic. During the study period, there were 6 outbreaks. All outbreaks were related to educational organizations. From 2010 to 2017, the hepatitis A vaccination rate of children in Hubei Province was over 90%. The number of hepatitis A new cases predicted by ARIMA model continued to decline, and it reduced to 484 cases in 2030, with a predicted incidence rate below 1/100 000. Conclusions From 2004 to 2019, the prevention and control measures of hepatitis A are effective. In the future, it is necessary to strengthen the comprehensive prevention and control measures for the rural population, especially for the middle-aged farmers, while doing a good job in the immunization plan of children. The occurrence of hepatitis A cannot be eliminated in 2030, but current prevention measures can further reduce the harm of the disease. -
Key words:
- Hepatitis A /
- Epidemiological characteristics /
- Prediction
-

图 1 2004―2019年湖北省甲肝报告新发病例数和发病率(1/10万)
Figure 1. Reported new case number and incidence of Hepatitis A in Hubei from 2004 to 2019 (1/100 000)

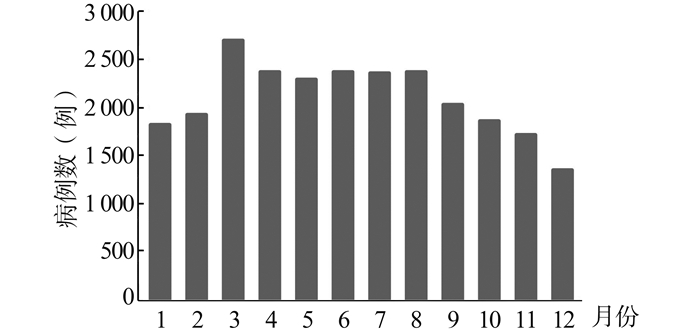
图 2 2004―2019年湖北省甲肝新发病例月分布
Figure 2. Monthly distribution of Hepatitis A new reported cases number in Hubei from 2004 to 2019

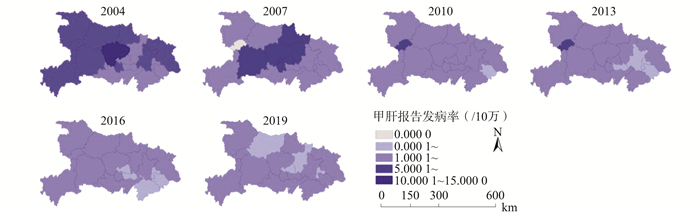
图 3 2004―2019年湖北省甲肝发病率地区差别
Figure 3. Regional difference of Hepatitis A incidence in Hubei from 2004 to 2019

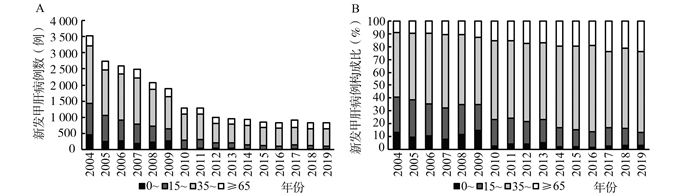
图 4 2004―2019年湖北省报告甲肝新发病例年龄及其构成变化
Figure 4. Reported new case number and proportion change of Hepatitis A in Hubei from 2004 to 2019

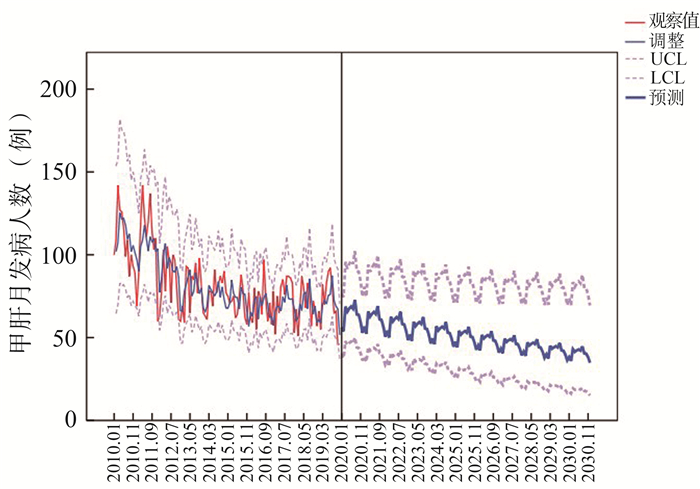
图 5 2010-2019湖北省甲肝发病人数建立的ARIMA(1, 1, 1)(1, 0, 1)模型预测结果
Figure 5. Prediction results of ARIMA (1, 1, 1) (1, 0, 1) model of hepatitis A patients number in Hubei from 2010 to 2019
表 1 湖北省2010-2017年出生儿童HepA接种率
Table 1. Coverage rates of Hepatitis A vaccination among children born in Hubei from 2010 to 2017
出生年份 儿童数 接种数 接种率(%) 2010 671 781 617 344 91.90 2011 740 673 720 180 97.23 2012 795 366 777 225 97.72 2013 718 512 708 806 98.65 2014 717 925 714 004 99.45 2015 684 194 665 072 97.21 2016 761 673 738 022 96.89 2017 715 913 709 095 99.05 合计 5 806 037 5 649 748 97.31  下载: 导出CSV
下载: 导出CSV
-
[1] 李燕婷.上海市甲型和乙型病毒性肝炎防治工作回顾[J].上海预防医学, 2019, 31(1):41-45. DOI: 10.19428/j.cnki.sjpm.2019.19242.Li YT. Review of prevention and treatment of hepatitis A and B in Shanghai[J]. Shanghai preventive medicine, 2019, 31(1):41-45. DOI: 10.19428/j.cnki.sjpm.2019.19242. [2] 中华人民共和国传染病防治法[M].法律出版社.全国人民代表大会常务委员会, 1989.Law of the People's Republic of China on the prevention and control of infectious diseases[M]. Legal Press.Standing Committee of the National People's Congress, 1989. [3] WHO. Media Centre. Hepatitis A.[EB/OL]. (2020-07-27)[2020-09-08] https://www.who.int/zh/news-room/fact-sheets/detail/hepatitis-a. [4] 中华人民共和国卫生部. WS298-2008.甲型病毒性肝炎诊断标准[S]. 2009.Ministry of health of the People's Republic of China. WS298-2008. Diagnostic criteria for hepatitis A[S]. 2009. [5] 徐志一, 汪萱怡, 赵守军.甲型肝炎减毒活疫苗保护效果与应用策略研究[J].中华流行病学杂志, 2002, 23(5):71-73. DOI: 10.3760/j.issn:0254-6450.2002.05.019.Xu ZY, Wang XY, Zhao SJ. Study on the protective effect and application strategy of live attenuated hepatitis A vaccine[J]. Chin J Epidemiol, 2002, 23(5):71-73. DOI: 10.3760/j.issn:0254-6450.2002.05.019. [6] 沈忠周, 马帅, 曲翌敏, 等. ARIMA模型在我国法定传染病报告数中的应用[J].中华流行病学杂志, 2017, 38(12):1708-1712. DOI: 10.3760/cma.j.issn.0254-6450.2017.12.025.Shen ZZ, Ma S, Qu YM, et al. The application of ARIMA model in the number of statutory infectious diseases reports in China[J]. Chin J Epidemiol, 2017, 38(12):1708-1712. DOI: 10.3760/cma.j.issn.0254-6450.2017.12.025. [7] 庄辉.全球消除病毒性肝炎策略[J].肝博士, 2016(5):1. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=gbs201605001Zhuang H. Global strategy to eliminate viral hepatitis[J]. Dr. Gan, 2016(5):1. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=gbs201605001 [8] 董瑞.全面二孩政策下人口结构及其对房价的影响研究[D].西安: 西安科技大学, 2019.Dong R. Population structure and its impact on housing prices under the comprehensive two child policy[D]. Xi'an: Xi'an University of science and technology, 2019. [9] 谭超, 李海, 王学燕, 等. 2004-2015年广西甲型肝炎流行病学特征分析[J].应用预防医学, 2016, 22(3):232-234. DOI: 10.3969/j.issn.1673-758X.2016.03.013.Tan C, Li H, Wang XY, et al. Epidemiological characteristics of hepatitis A in Guangxi from 2004 to 2015[J]. Applied preventive medicine, 2016, 22(3):232-234. DOI: 10.3969/j.issn.1673-758X.2016.03.013. [10] Melgaço JG, Morgado LN, Santiago MA. A single dose of inactivated hepatitis A vaccine promotes HAV-specific memory cellular response similar to that induced by a natural infection[J]. Vaccine, 2015, 32(33):3813-3820. DOI: 10.1016/j.vaccine.2015.06.099 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 557
- HTML全文浏览量: 222
- PDF下载量: 50
- 被引次数: 0